

Diagnostics of infrapatellar saphenous neuralgia-a reversible cause of chronic anteromedial pain following knee surgery
- PMID: 34342695
- PMCID: PMC8330472
- DOI: 10.1007/s00330-021-08184-2
Diagnostics of infrapatellar saphenous neuralgia-a reversible cause of chronic anteromedial pain following knee surgery
Abstract
Objectives: To evaluate the impact of diagnostic nerve block and ultrasound findings on therapeutic choices and predict the outcome after concomitant surgery in patients with suspected neuropathy of the infrapatellar branch of the saphenous nerve (IPBSN).
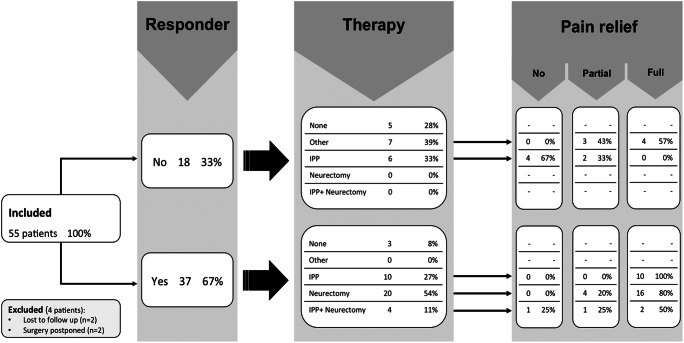
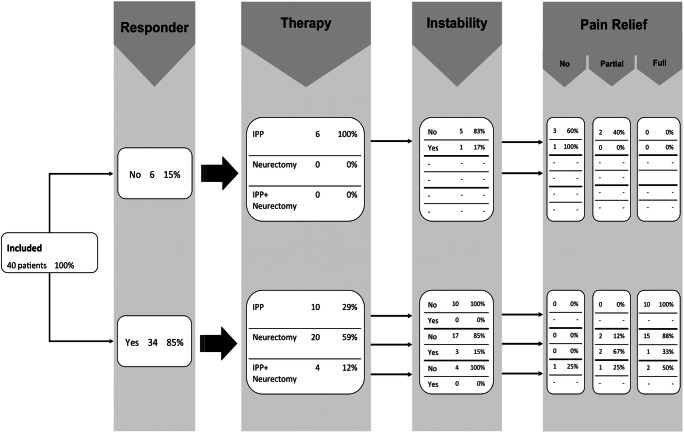
Methods: Fifty-five patients following knee surgery with suspicion of IPBSN neuralgia were retrospectively included. Ultrasound reports were assessed for neuroma and postsurgical scarring (yes/no). Responders and non-responders were assigned following anesthetic injection of the IPBSN. The type of procedure (neurectomy/interventional pain procedure/other than nerve-associated therapy) and pain score at initial follow-up were recorded and patients were assigned as positive (full pain relief) or negative (partial/no pain relief) to therapeutic nerve treatment. Factors associated with a relevant visual analog scale (VAS) reduction were assessed using uni- and multivariate logistic regression models and chi-square for quantitative and qualitative variables (p ≤ 0.05).
Results: Responders (37/55) more often had an entrapment or an evident neuroma of the IPBSN (97% vs. 6%). A positive Hoffmann-Tinel sign (p = 0.002) and the absence of knee joint instability (p = 0.029) predicted a positive response of the diagnostic nerve block (90%; 26/29). In the follow-up after therapeutic nerve treatment, all patients with full pain relief showed neuromas or entrapment of the IPBSN. Patients negatively responding to therapeutic nerve treatment more frequently showed an additional knee joint instability (25% vs. 4%).
Conclusion: Selective denervation for neuropathic knee pain is beneficial in selected patients with significant VAS reduction after diagnostic nerve block. Non-responders following diagnostic nerve block but sonographic evidence of IPBSN pathologies need to be evaluated for other causes such as knee joint instability.
Key points: • Sonographic diagnosis of neuroma or entrapment of the IPBSN is frequently seen in patients with anteromedial knee pain and leads to a good response to diagnostic nerve block following knee surgery. • The vast majority of patients with clinical signs of IPBSN neuropathy and response to a diagnostic nerve block sustained full pain relief following therapeutic nerve treatment. • Patients not responding to therapeutic IPBSN treatment have to be evaluated for other causes of anteromedial knee pain such as knee joint instability.
Keywords: Knee surgery; Nerve block; Saphenous nerve; Total knee arthroplasty; Ultrasound.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
