

New risk stratification after colorectal polypectomy reduces burden of surveillance without increasing mortality
- PMID: 34343405
- PMCID: PMC8498405
- DOI: 10.1002/ueg2.12119
New risk stratification after colorectal polypectomy reduces burden of surveillance without increasing mortality
Abstract
Background: The 2020 postpolypectomy surveillance guideline update of European Society for Gastrointestinal Endoscopy defines a more restrictive group of individuals in need for surveillance 3 years after colonoscopy.
Aim: The aim of this cohort study was to validate the new guideline recommendation.
Methods: Based on a national quality assurance program, we compared the 2020 risk group definition with the previous 2013 recommendations for their strength of association with (1) colorectal cancer death, and (2) all-cause death.
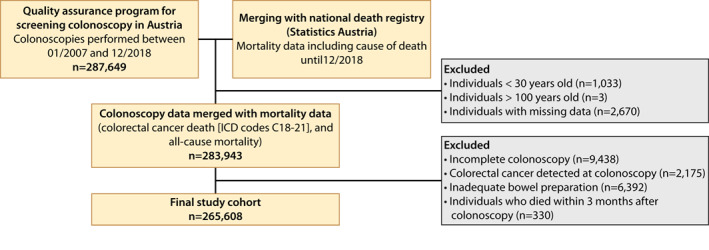
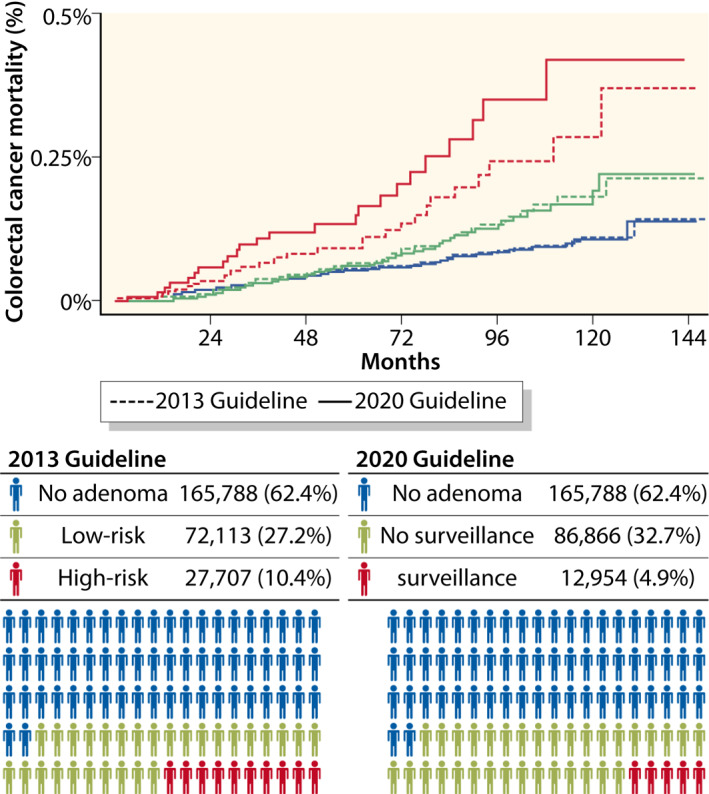
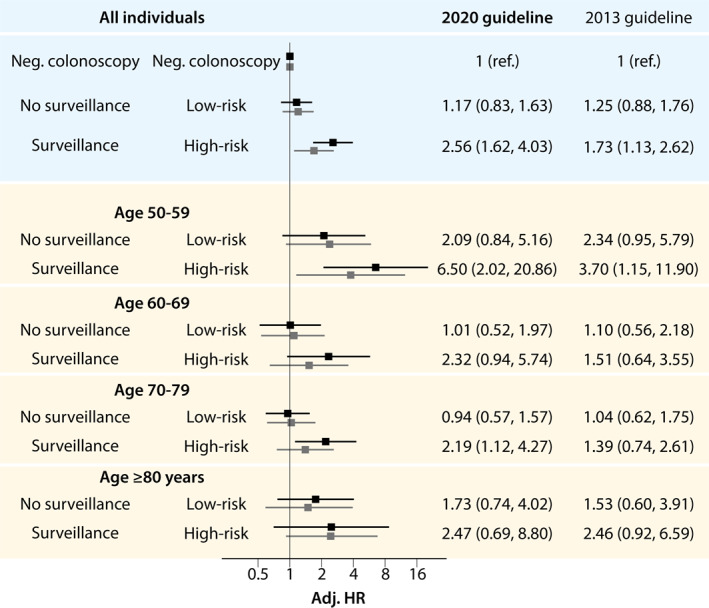
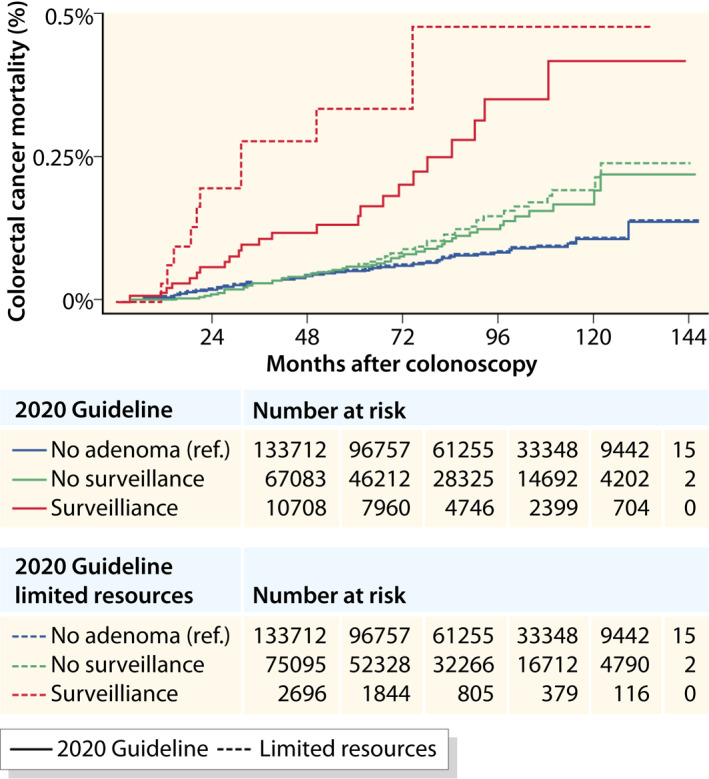
Results: A total of 265,608 screening colonoscopies were included in the study. Mean age was 61.1 years (SD ±9.0), and 50.6% were women. During a mean follow-up of 59.3 months (SD ±35.0), 170 CRC deaths and 7723 deaths of any cause were identified. 62.4% of colonoscopies were negative and 4.9% were assigned to surveillance after 3 years according to the 2020 guidelines versus 10.4% following the 2013 guidelines, which corresponds to a relative reduction in colonoscopies by 47%. The strength of association with CRC mortality was markedly higher with the 2020 surveillance group as compared to the 2013 guidelines (HR 2.56, 95% CI 1.62-4.03 vs. HR 1.73, 95% CI 1.13-2.62), while the magnitude of association with CRC mortality for low risk individuals was lower (HR 1.17, 95% CI 0.83-1.63 vs. 1.25, 95% CI 0.88-1.76).
Conclusions: Adherence to the updated guidelines reduces the burden of surveillance colonoscopies by 47% while preserving the efficacy of surveillance in preventing CRC mortality.
Keywords: CRC; cancer; colonoscopy; colorectal cancer; mortality; polypectomy; risk-stratification; screening; surveillance.
© 2021 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC. on behalf of United European Gastroenterology.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin. 2018;68 (6):394–424. - PubMed
-
- Cottet V, Jooste V, Fournel I, Bouvier AM, Faivre J, Bonithon‐Kopp C. Long‐term risk of colorectal cancer after adenoma removal: a population‐based cohort study. Gut. 2012;61(8):1180–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
