

Coincidental light chain induced proximal tubulopathy with lupus nephritis: a case report and review of the literature
- PMID: 34344460
- PMCID: PMC8335886
- DOI: 10.1186/s13256-021-02990-4
Coincidental light chain induced proximal tubulopathy with lupus nephritis: a case report and review of the literature
Abstract
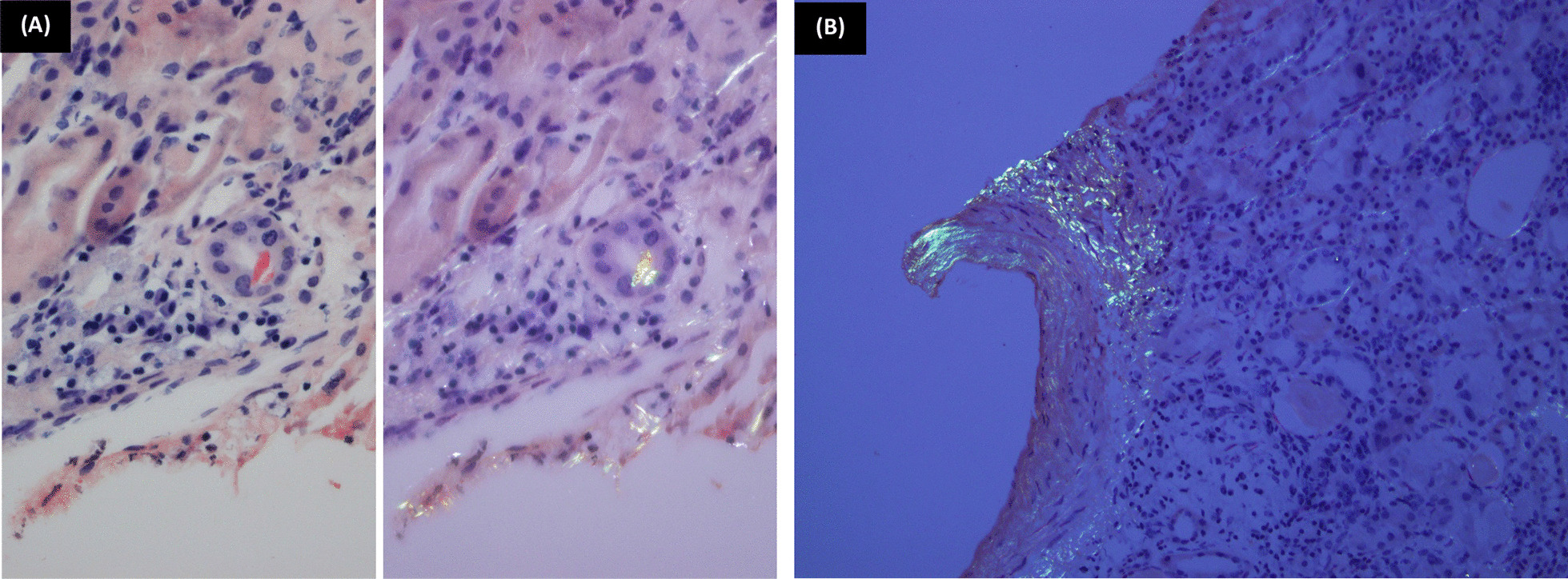
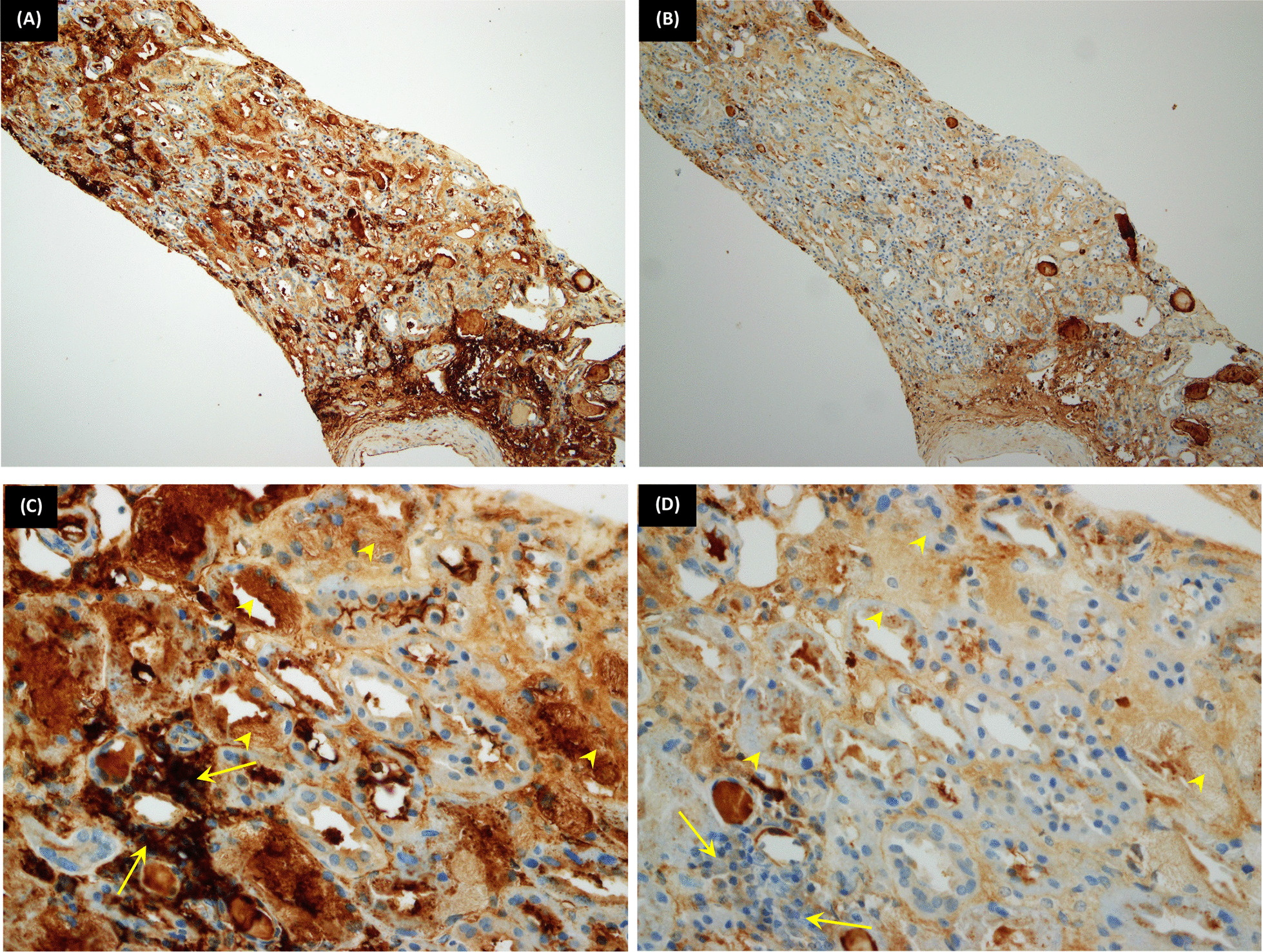
Background: We report a case of light chain proximal tubulopathy associated with lupus nephritis in a patient known to have systemic lupus erythematosus. The kidney can be injured in several ways in any of these disorders. Light chain proximal tubulopathy is a rare form of renal tubular injury that may occur in and complicate plasma cell dyscrasia, characterized by cytoplasmic inclusions of the monoclonal light chain within proximal tubular cells. Lupus nephritis is a common form of renal injury as it occurs in about 25-50% of adult patients with systemic lupus erythematosus.
Case presentation: We present a 57-year-old African patient known to have systemic lupus erythematosus and hypertension presented with a new complaint of microscopic hematuria. A renal biopsy was performed and revealed lupus nephritis class II concurrently associated with light chain induced proximal tubulopathy. A subsequent bone marrow biopsy was performed, which revealed multiple myeloma.
Conclusions: We report a case of coincidental lupus nephritis and proximal tubulopathy featuring a combined constellation of rare histopathological features that might add to the relationship between systemic lupus and paraproteinemia.
Keywords: Free light chain; Lupus nephritis; Paraproteinemia; Plasma cell dyscrasia; Proximal tubulopathy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
