

Donor derived cell free DNA% is elevated with pathogens that are risk factors for acute and chronic lung allograft injury
- PMID: 34344623
- PMCID: PMC8571060
- DOI: 10.1016/j.healun.2021.05.012
Donor derived cell free DNA% is elevated with pathogens that are risk factors for acute and chronic lung allograft injury
Abstract
Background: Acute and chronic forms of lung allograft injury are associated with specific respiratory pathogens. Donor-derived cell free DNA (ddcfDNA) has been shown to be elevated with acute lung allograft injury and predictive of long-term outcomes. We examined the %ddcfDNA values at times of microbial isolation from bronchoalveolar lavage (BAL).
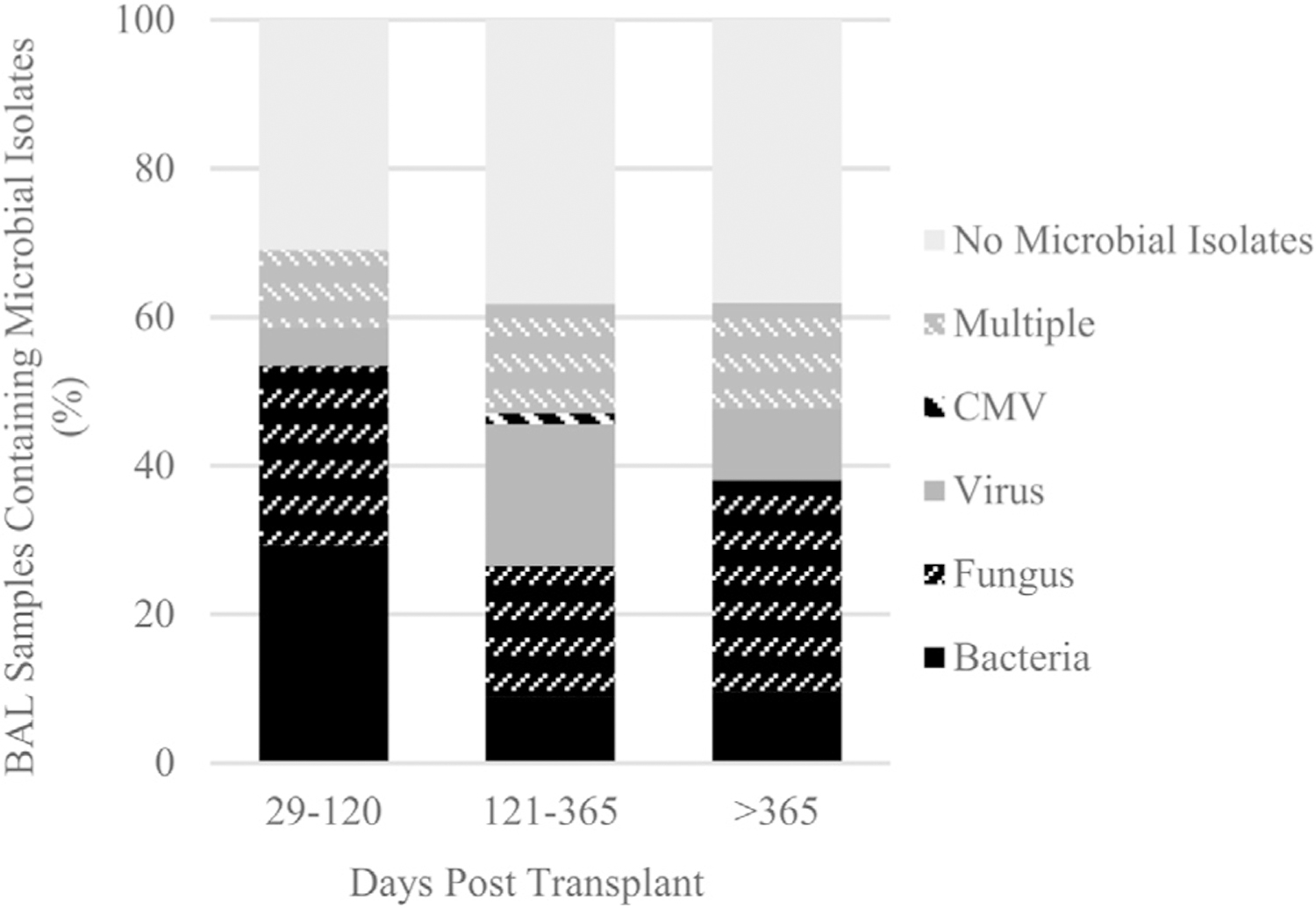
Methods: Two hundred and six BAL samples from 51 Lung Transplant Recipients (LTRs) with concurrently available plasma %ddcfDNA were analyzed along with microbiology and histopathology. Microbial species were grouped into bacterial, fungal, and viral and "higher risk" and "lower risk" cohorts based on historical association with downstream allograft dysfunction. Analyses were performed to determine pathogen category association with %ddcfDNA, independent of inter-subject variability.
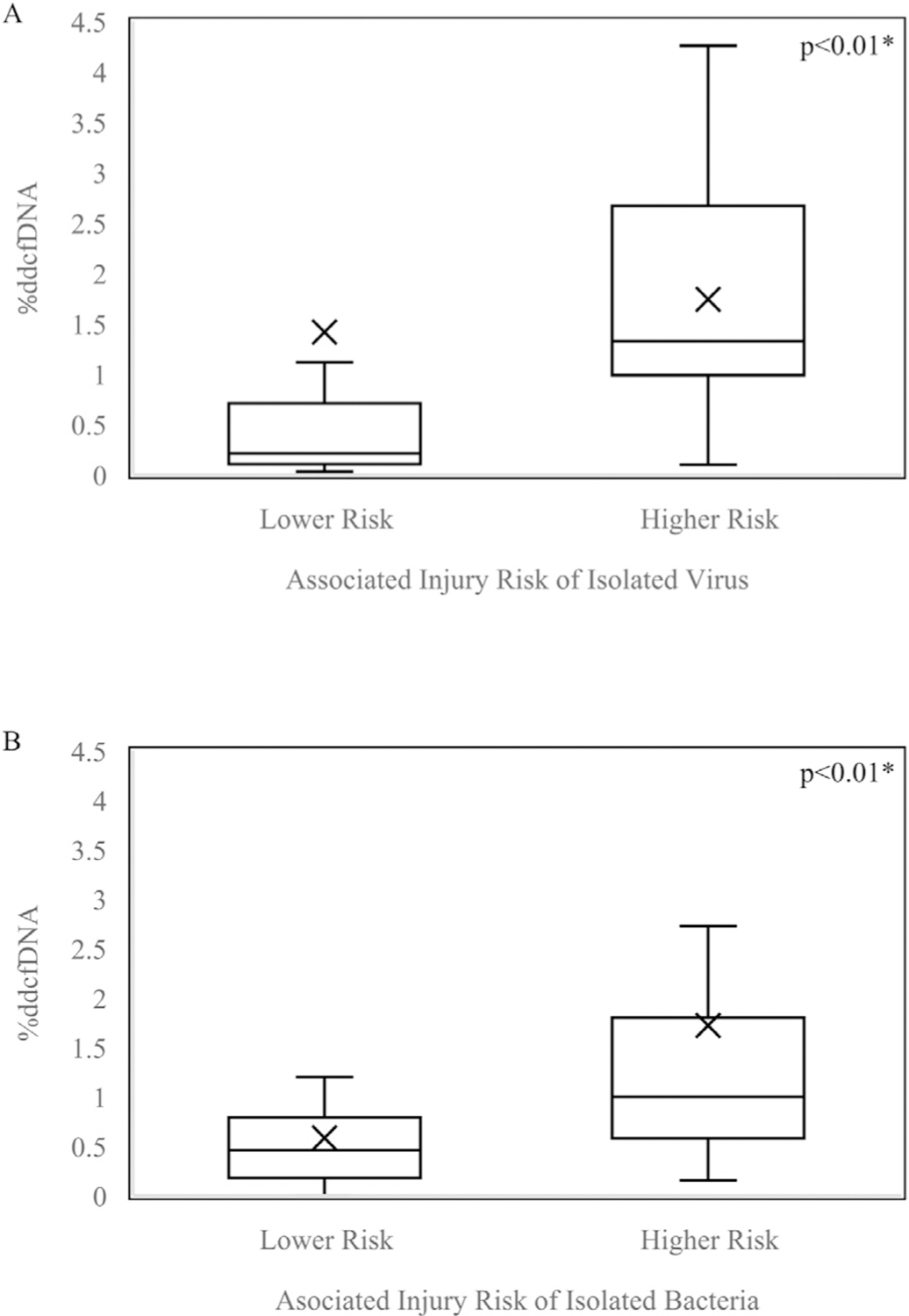
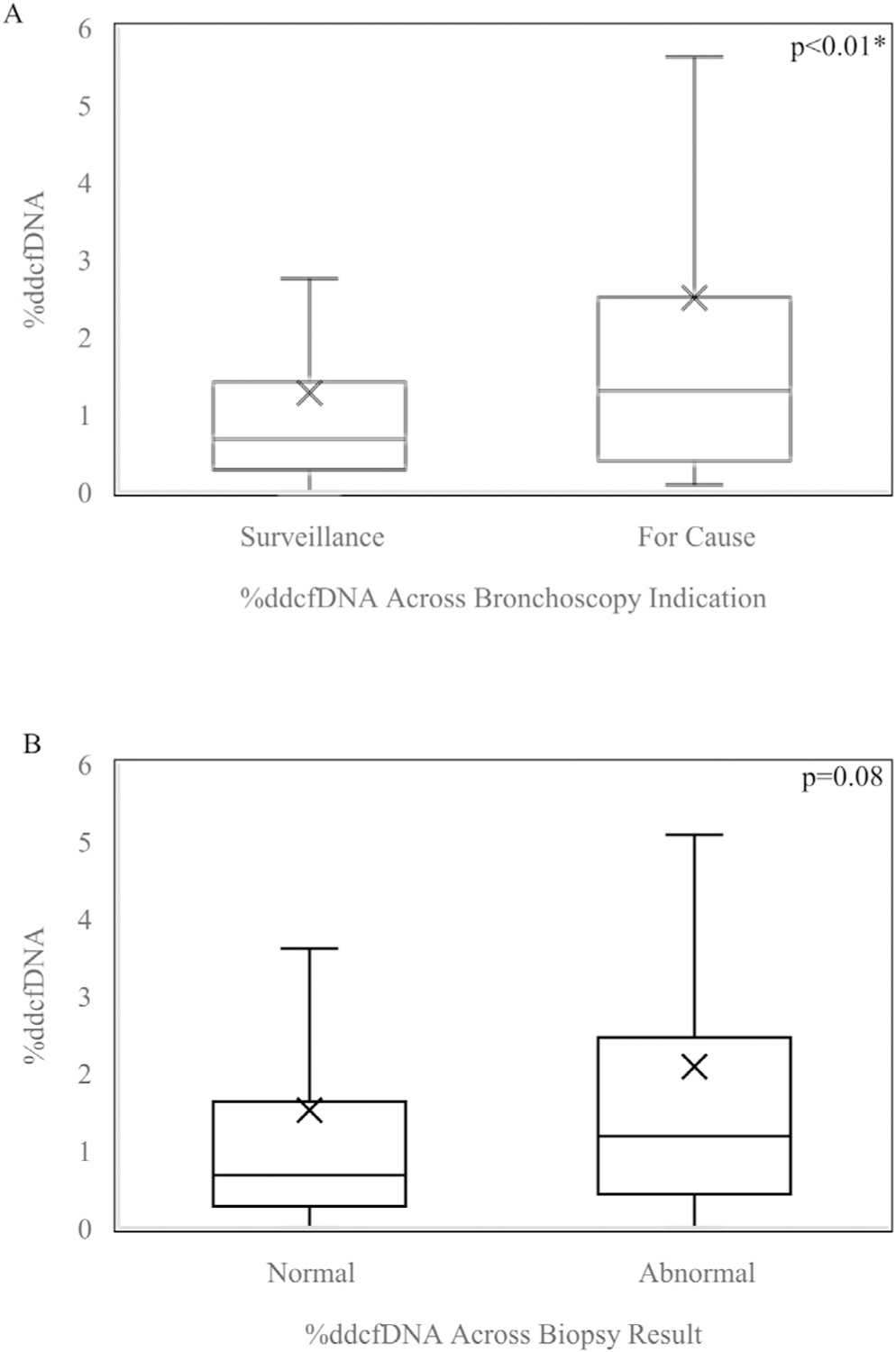
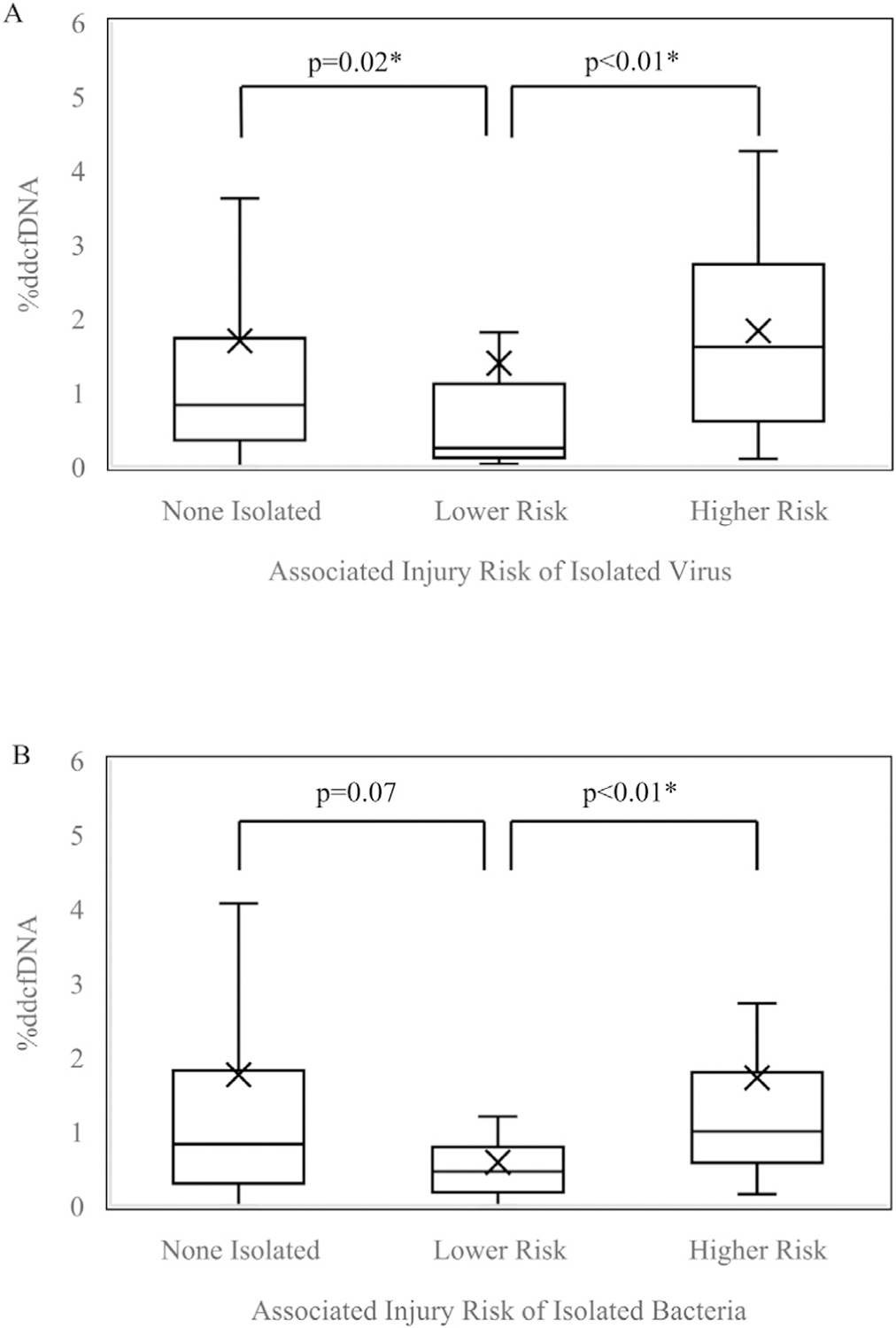
Results: Presence of microbial isolates in BAL was not associated with elevated %ddcfDNA compared to samples without isolates. However, "higher risk" bacterial and viral microbes showed greater %ddcfDNA values than lower risk species (1.19% vs. 0.65%, p < 0.01), independent of inter-subject variability. Histopathologic abnormalities concurrent with pathogen isolation were associated with higher %ddcfDNA compared to isolation episodes with normal histopathology (medians 1.23% and 0.66%, p = 0.05). Assessments showed no evidence of correlation between histopathology or bronchoscopy indication and presence of higher risk vs. lower risk pathogens.
Conclusion: %ddcfDNA is higher among cases of microbial isolation with concurrent abnormal histopathology and with isolation of higher risk pathogens known to increase risk of allograft dysfunction. Future studies should assess if %ddcfDNA can be used to stratify pathogens for risk of CLAD and identify pathogen associated injury prior to histopathology.
Keywords: cfDNA; chronic lung allograft dysfunction; lung transplantation; transplant infection.
Copyright © 2021 International Society for Heart and Lung Transplantation. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
