

Cerebral malaria: insight into pathology from optical coherence tomography
- PMID: 34344903
- PMCID: PMC8333417
- DOI: 10.1038/s41598-021-94495-9
Cerebral malaria: insight into pathology from optical coherence tomography
Abstract
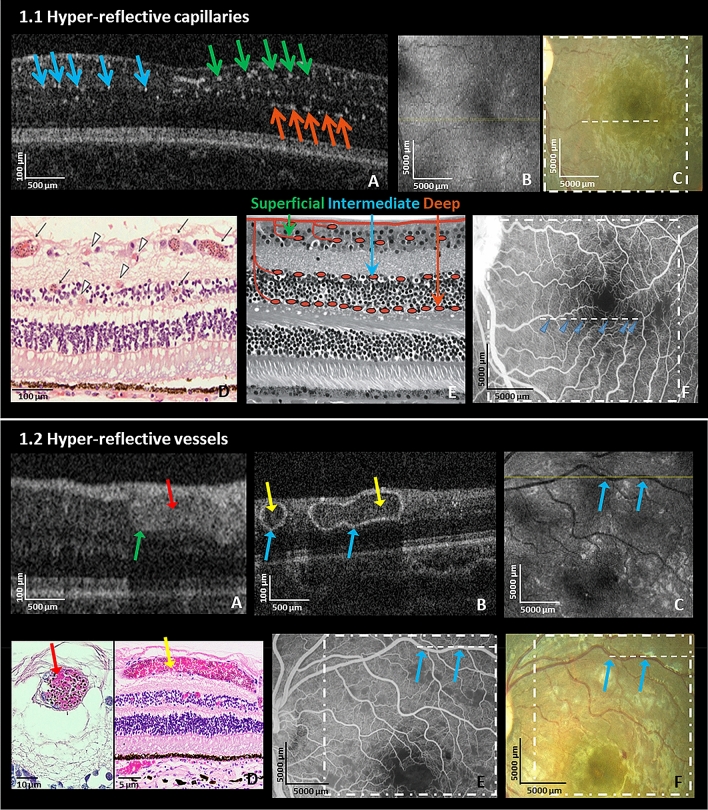
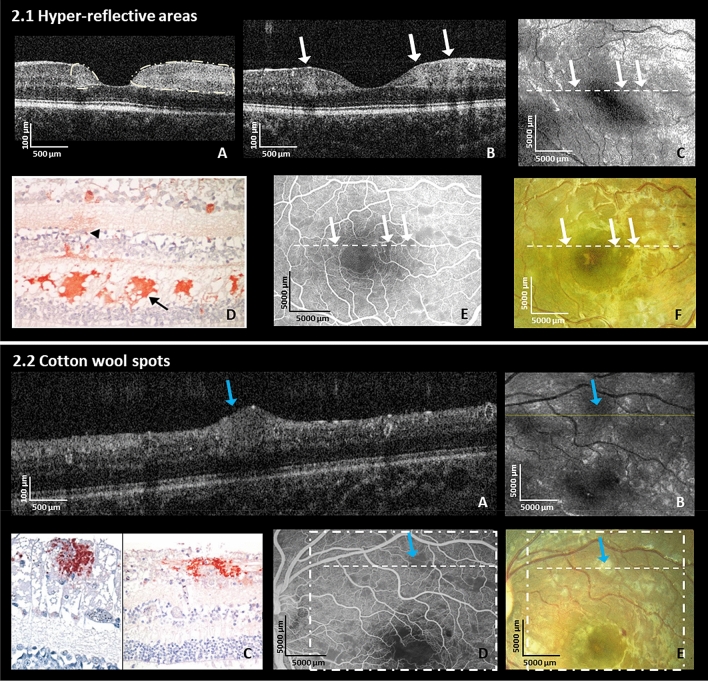
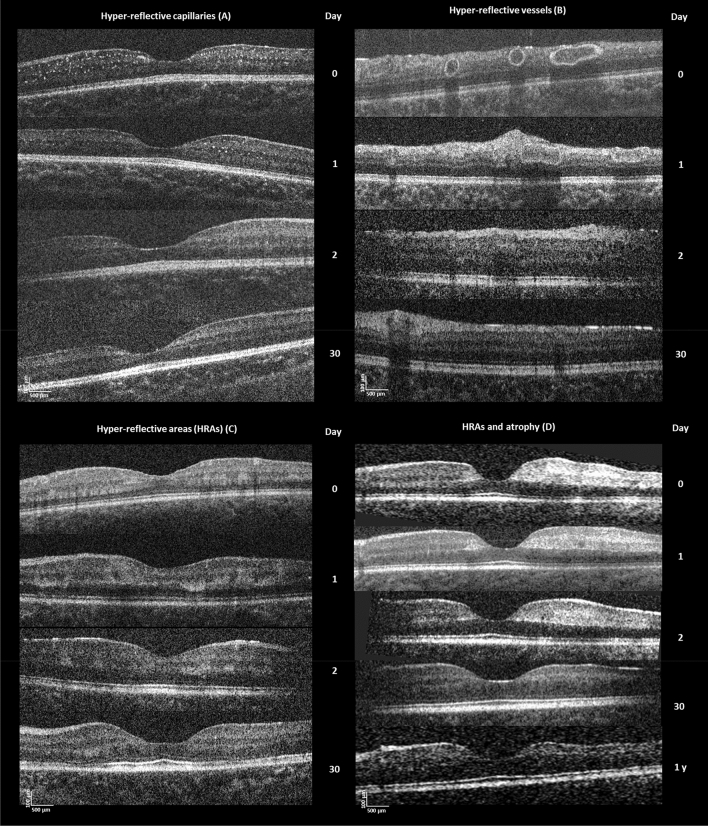
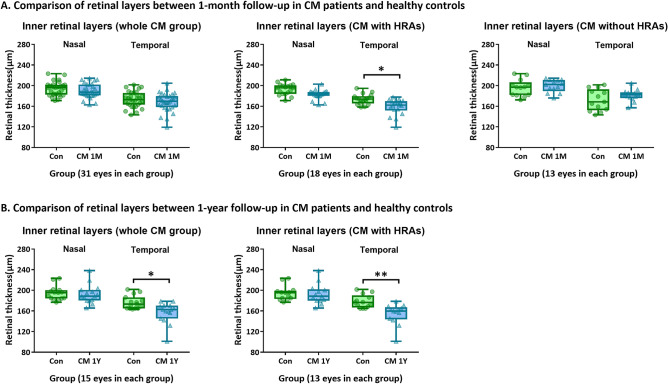
We aimed to investigate structural retinal changes in malarial retinopathy (MR) using hand-held optical coherence tomography (HH-OCT) to assess its diagnostic potential. Children with MR (n = 43) underwent ophthalmoscopy, fluorescein angiography and HH-OCT during admission, 1-month (n = 31) and 1-year (n = 8) post-discharge. Controls were comatose patients without malaria (n = 6) and age/sex-matched healthy children (n = 43). OCT changes and retinal layer thicknesses were compared. On HH-OCT, hyper-reflective areas (HRAs) were seen in the inner retina of 81% of MR patients, corresponding to ischaemic retinal whitening on fundus photography. Cotton wool spots were present in 37% and abnormal hyper-reflective dots, co-localized to capillary plexus, in 93%. Hyper-reflective vessel walls were present in 84%, and intra-retinal cysts in 9%. Vascular changes and cysts resolved within 48 h. HRAs developed into retinal thinning at 1 month (p = 0.027) which was more pronounced after 1 year (p = 0.009). Ischaemic retinal whitening is located within inner retinal layers, distinguishing it from cotton wool spots. Vascular hyper-reflectivity may represent the sequestration of parasitized erythrocytes in vessels, a key CM feature. The mechanisms of post-ischemic retinal atrophy and cerebral atrophy with cognitive impairment may be similar in CM survivors. HH-OCT has the potential for monitoring patients, treatment response and predicting neurological deficits.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Postels DG, Chimalizeni YF, Mallewa M, Boivin MJ, Seydel KB. Pediatric cerebral malaria: A scourge of Africa. Future Neurol. 2013;8:67–85. doi: 10.2217/fnl.12.84. - DOI
-
- WHO . World Malaria Report 2020. WHO; 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
