

A rare, pediatric, fourth-ventricular, anaplastic astrocytoma
- PMID: 34345330
- PMCID: PMC8319461
- DOI: 10.1016/j.radcr.2021.06.050
A rare, pediatric, fourth-ventricular, anaplastic astrocytoma
Abstract
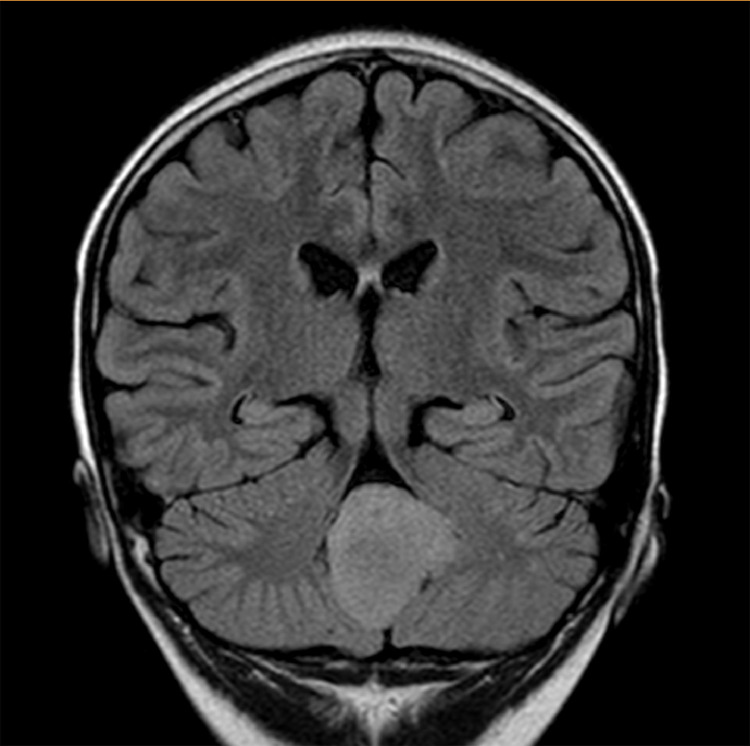
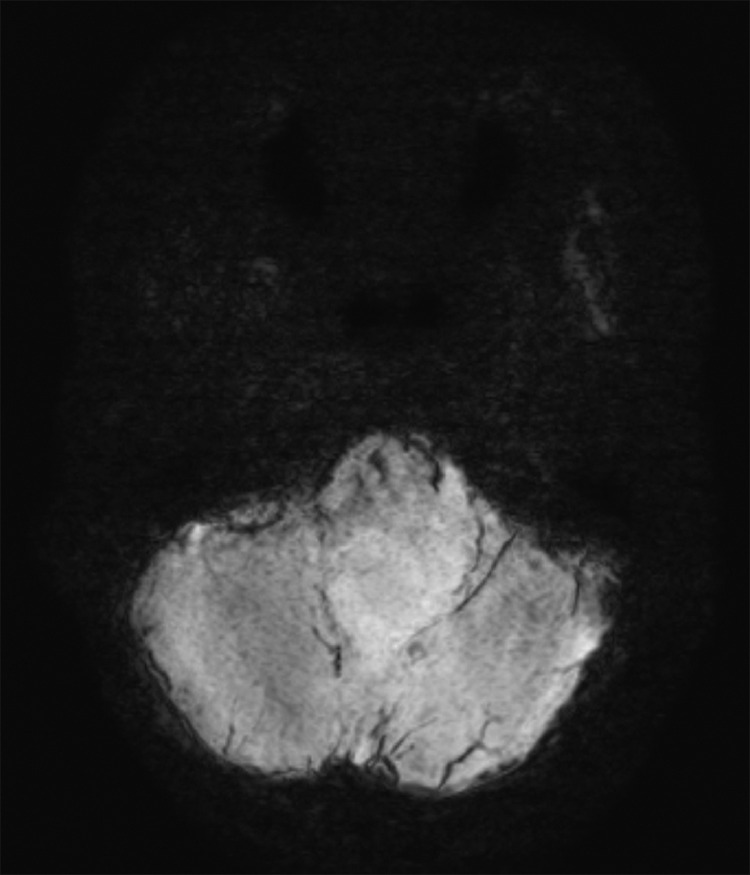
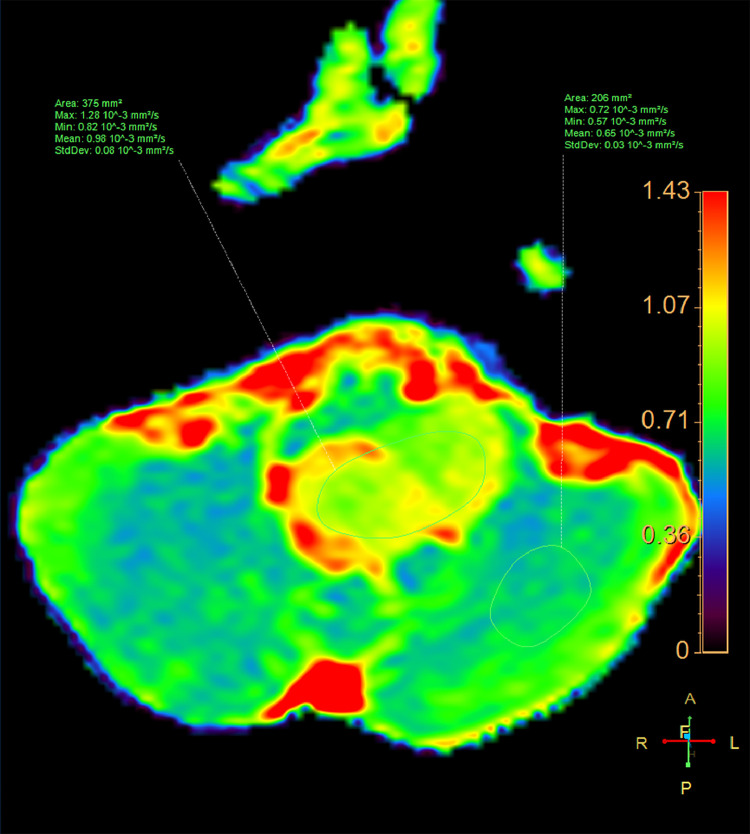
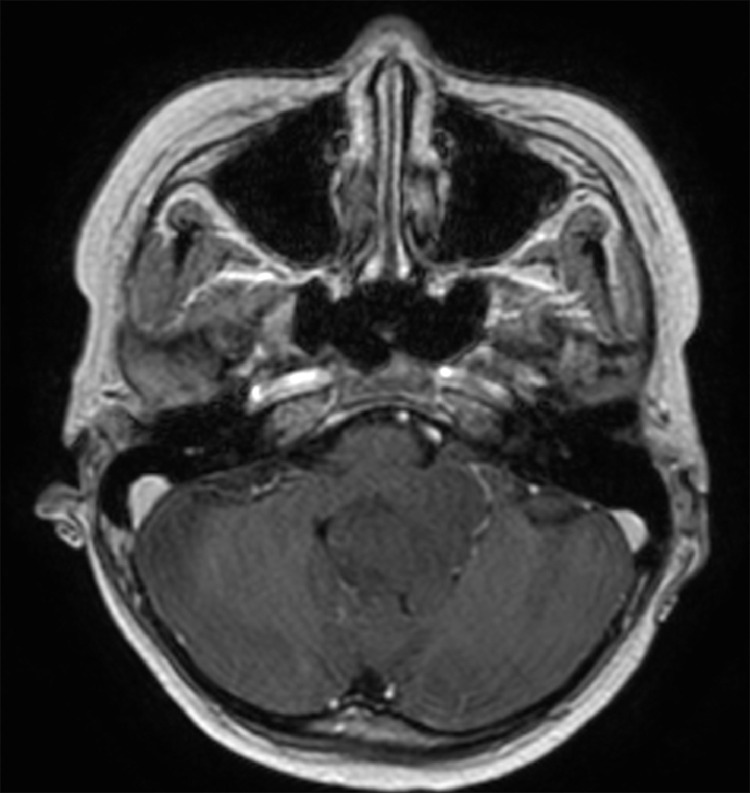
Anaplastic astrocytoma, a diffusely infiltrating, malignant, astrocytic, primary brain tumor, is most commonly observed between 30 and 50 years of age. Anaplastic astrocytomas are now classified as WHO grade III lesions, with imaging characteristics and prognosis between diffuse low-grade astrocytomas (WHO grade II) and glioblastomas (WHO IV). Anaplastic astrocytoma can appear mostly in the cerebrum followed by cerebellum. However, it is rarely observed in the fourth ventricle. In this article, we aimed to describe an uncommon case of a pediatric, fourth-ventricular, anaplastic astrocytoma. A 9-year-old male who underwent MRI brain then adopted gross-total tumor eradication. The final histopathology findings were consistent with an anaplastic astrocytoma.
Keywords: Anaplastic astrocytoma; Children; Extraparenchymal; Intraventricular.
© 2021 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures


References
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–820. - PubMed
-
- Mechtler L. Neuroimaging in neuro-oncology. Neurol Clin. 2009;27(1):171–201. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
