

Survival with low- and high-flux dialysis
- PMID: 34345415
- PMCID: PMC8323142
- DOI: 10.1093/ckj/sfaa233
Survival with low- and high-flux dialysis
Abstract
Background: Besides advances in haemodialysis (HD), mortality rates are still high. The effect of the different types of HD membranes on survival is still a controversial issue. The aim of this COSMOS (Current management Of Secondary hyperparathyroidism: a Multicentre Observational Study) analysis was to survey, in HD patients, the relationship between the use of conventional low- or high-flux membranes and all-cause and cardiovascular mortality.
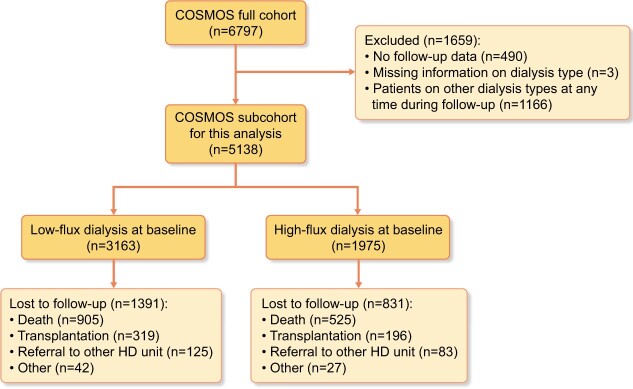
Methods: COSMOS is a multicentre, open-cohort, 3-year prospective study, designed to evaluate mineral and bone disorders in the European HD population. The present analysis included 5138 HD patients from 20 European countries, 3502 randomly selected at baseline (68.2%), plus 1636 new patients with <1 year on HD (31.8%) recruited to replace patients who died, were transplanted, switched to peritoneal dialysis or lost to follow-up by other reasons. Cox-regression analysis with time-dependent variables, propensity score matching and the use of an instrumental variable (facility-level analysis) were used.
Results: After adjustments using three different multivariate models, patients treated with high-flux membranes showed a lower all-cause and cardiovascular mortality risks {hazard ratio (HR) = 0.76 [95% confidence interval (CI) 0.61-0.96] and HR = 0.61 (95% CI 0.42-0.87), respectively}, that remained significant after matching by propensity score for all-cause mortality (HR = 0.69, 95% CI 0.52-0.93). However, a facility-level analysis showed no association between the case-mix-adjusted facility percentage of patients dialysed with high-flux membranes and all-cause and cardiovascular mortality.
Conclusions: High-flux dialysis was associated with a lower relative risk of all-cause and cardiovascular mortality. However, dialysis facilities using these dialysis membranes to a greater extent did not show better survival.
Keywords: chronic haemodialysis; dialysis; dialysis membranes; mortality; mortality risk.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures

References
-
- Kramer A, Stel V, Zoccali C. et al. An update on renal replacement therapy in Europe: ERA-EDTA registry data from 1997 to 2006. Nephrol Dial Transplant 2009; 24: 3557–3566 - PubMed
-
- Panichi V, Rizza GM, Paoletti S. et al.; on behalf of the RISCAVID Study Group. Chronic inflammation and mortality in haemodialysis: effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol Dial Transplant 2008; 23: 2337–2343 - PubMed
LinkOut - more resources
Full Text Sources
