

Thoracic dorsal arachnoid web with rapid onset of symptoms: A report of two cases and brief review of the literature
- PMID: 34345464
- PMCID: PMC8326092
- DOI: 10.25259/SNI_339_2021
Thoracic dorsal arachnoid web with rapid onset of symptoms: A report of two cases and brief review of the literature
Abstract
Background: Thoracic arachnoid webs are a rare entity and can be challenging to diagnose with sometimes subtle radiographic findings. Arachnoid webs can cause severe cord compression with associated syrinx and resulting myelopathy, weakness, sensory loss, and bowel/bladder dysfunction. There have been a little over 60 cases total reported in the literature with only one systematic review. The cases presented here have unique features including rapid onset of symptoms, symptomatic syrinx extending into the cervical spine, and intraoperative syrinx drainage, all of which are quite rare in the current published literature for arachnoid webs.
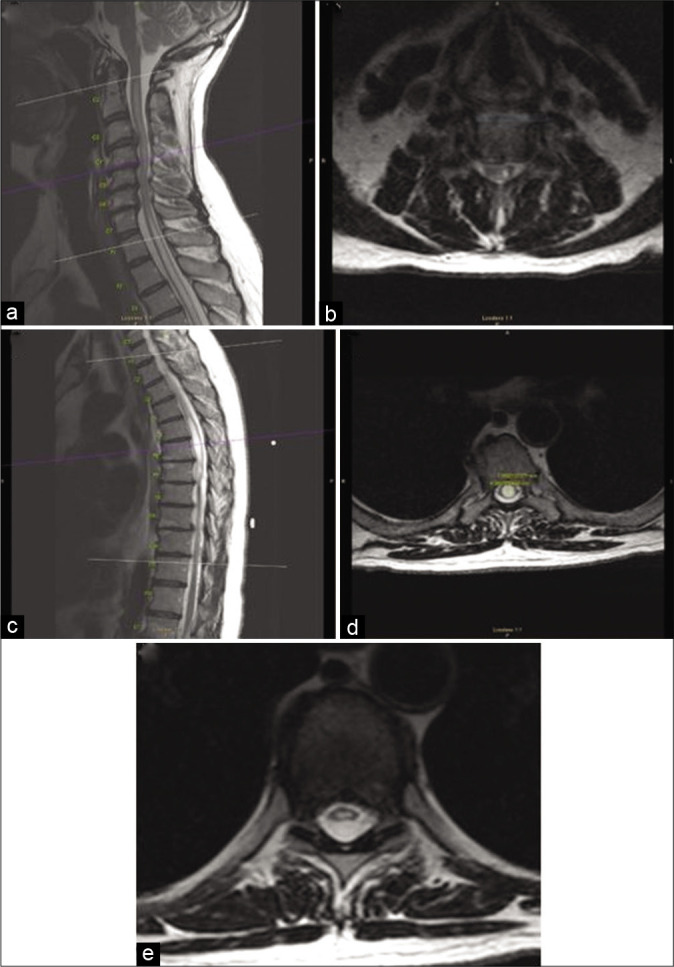
Case description: Here, we present two patients, a 73-year-old man and 58-year-old man presenting with different symptoms and timing of symptom progression but both with "scalpel sign" and associated syrinx present on their MRIs. Each patient underwent a laminectomy with resection of arachnoid web with complete resolution of symptoms in the first case and significant improvement in the second case. Postoperative imaging in both cases showed almost complete resolution of the syrinx.
Conclusion: Early clinical evaluation and workup followed by early surgical treatment can lead to dramatic improvement in outcomes after surgery. For patients that are symptomatic from an associated syrinx, a midline myelotomy to facilitate drainage can be considered to be done concomitantly with the arachnoid web resection.
Keywords: Arachnoid web; Dorsal; Review; Spine; Surgery; Thoracic.
Copyright: © 2021 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures




References
-
- Aljuboori Z, Boakye M. Surgical release of a dorsal thoracic arachnoid web. World Neurosurg. 2020;143:289. - PubMed
-
- Brasil P, Pereira L, Távora D, Camara A, Filho CM, Coimbra P. Imaging findings in dorsal thoracic arachnoid web and the differential diagnosis of “scalpel sign”. Neurographics. 2020;10:96–102.
-
- Chang H, Nagai A, Oya S, Matsui T. Dorsal spinal arachnoid web diagnosed with the quantitative measurement of cerebrospinal fluid flow on magnetic resonance imaging. J Neurosurg Spine. 2014;20:227–33. - PubMed
Publication types
LinkOut - more resources
Full Text Sources