

Descriptive analysis of long COVID sequelae identified in a multidisciplinary clinic serving hospitalised and non-hospitalised patients
- PMID: 34345629
- PMCID: PMC8091683
- DOI: 10.1183/23120541.00205-2021
Descriptive analysis of long COVID sequelae identified in a multidisciplinary clinic serving hospitalised and non-hospitalised patients
Abstract
Background: There are emerging data of long-term effects of coronavirus disease 2019 (COVID-19) comprising a diversity of symptoms. The aim of this study was to systematically describe and measure pulmonary and extra-pulmonary post-COVID-19 complications in relation to acute COVID-19 severity.
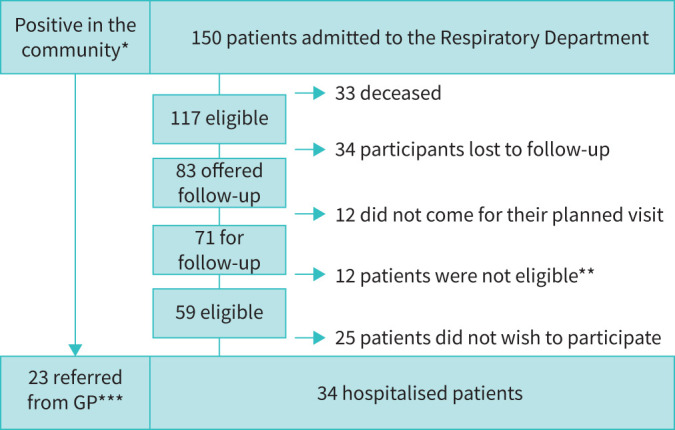
Methods: Patients attending a standard of care 3 months post-hospitalisation follow-up visit and those referred by their general practitioner because of persistent post-COVID-19 symptoms were included. Patients underwent symptomatic, quality of life, pulmonary (lung function and high-resolution computed tomography (HRCT)), cardiac (high-resolution ECG), physical (1-min sit and stand test (1-MSTST), handgrip strength, cardiopulmonary exercise testing (CPET)) and cognitive evaluations.
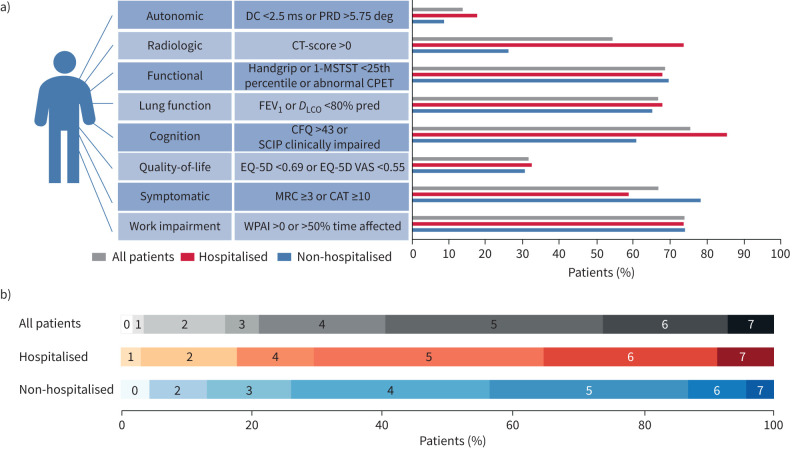
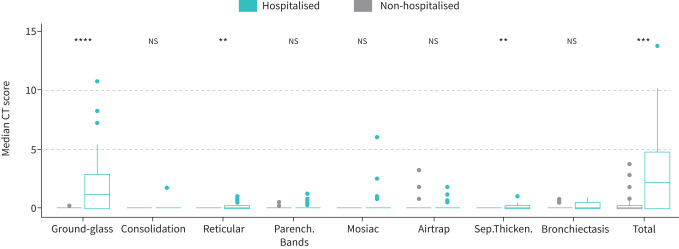
Results: All 34 hospitalised and 22 out of 23 non-hospitalised patients had ≥1 complaint or abnormal finding at follow-up. Overall, 67% of patients were symptomatic (Medical Research Council (MRC) ≥2 or COPD assessment test (CAT) ≥10), with no difference between hospitalised versus non-hospitalised patients. Pulmonary function (forced expiratory volume in 1 s (FEV1) or diffusing capacity of the lung for carbon monoxide (D LCO)) <80% of predicted) was impaired in 68% of patients. D LCO was significantly lower in those hospitalised compared to non-hospitalised (70.1±18.0 versus 80.2±11.2% predicted, p=0.02). Overall, 53% had an abnormal HRCT (predominantly ground-glass opacities) with higher composite computed tomography (CT) scores in hospitalised versus non-hospitalised patients (2.3 (0.1-4.8) and 0.0 (0.0-0.3), p<0.001). 1-MSTST was below the 25th percentile in almost half of patients, but no signs of cardiac dysfunction were found. Cognitive impairments were present in 59-66% of hospitalised and 31-44% of non-hospitalised patients (p=0.08).
Conclusion: Three months after COVID-19 infection, patients were still symptomatic and demonstrated objective respiratory, functional, radiological and cognitive abnormalities, which were more prominent in hospitalised patients. Our study underlines the importance of multidimensional management strategies in these patients.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: S. Johnsen has nothing to disclose. Conflict of interest: S.M. Sattler has nothing to disclose. Conflict of interest: K.W. Miskowiak reports personal feels from Lundbeck outside the submitted work. Conflict of interest: K. Kunalan has nothing to disclose. Conflict of interest: A. Victor has nothing to disclose. Conflict of interest: L. Pedersen has nothing to disclose. Conflict of interest: H.F. Andreassen has nothing to disclose. Conflict of interest: B.J. Jørgensen has nothing to disclose. Conflict of interest: H. Heebøll has nothing to disclose. Conflict of interest: M.B. Andersen has nothing to disclose. Conflict of interest: L. Marner has nothing to disclose. Conflict of interest: C. Hædersdal has nothing to disclose. Conflict of interest: H. Hansen has nothing to disclose. Conflict of interest: S. Ditlev has nothing to disclose. Conflict of interest: C. Porsbjerg has nothing to disclose. Conflict of interest: T.S. Lapperre has nothing to disclose.
Figures
Similar articles
-
Dyspnoea, lung function and CT findings 3 months after hospital admission for COVID-19.Eur Respir J. 2021 Apr 29;57(4):2003448. doi: 10.1183/13993003.03448-2020. Print 2021 Apr. Eur Respir J. 2021. PMID: 33303540 Free PMC article.
-
Physical Function and Association with Cognitive Function in Patients in a Post-COVID-19 Clinic-A Cross-Sectional Study.Int J Environ Res Public Health. 2023 May 18;20(10):5866. doi: 10.3390/ijerph20105866. Int J Environ Res Public Health. 2023. PMID: 37239592 Free PMC article.
-
Respiratory recovery trajectories after severe-to-critical COVID-19: a 1-year prospective multicentre study.Eur Respir J. 2023 Apr 1;61(4):2201532. doi: 10.1183/13993003.01532-2022. Print 2023 Apr. Eur Respir J. 2023. PMID: 36669777 Free PMC article.
-
[Morphological and functional sequelae after COVID-19 pneumonia].Radiologe. 2021 Oct;61(10):888-895. doi: 10.1007/s00117-021-00905-4. Epub 2021 Sep 16. Radiologe. 2021. PMID: 34529126 Free PMC article. Review. German.
-
Incidence and follow-up of persistent lung perfusion abnormalities as a result of suspected air trapping or microthrombosis in non-hospitalised COVID-19 patients during the early half of the pandemic - experience in a tertiary institution in South Afr.S Afr Med J. 2022 Nov 1;112(11):850-854. doi: 10.7196/SAMJ.2022.v112i11.16578. S Afr Med J. 2022. PMID: 36420721 Review.
Cited by
-
Cognitive Deficits in the Acute Phase of COVID-19: A Review and Meta-Analysis.J Clin Med. 2023 Jan 18;12(3):762. doi: 10.3390/jcm12030762. J Clin Med. 2023. PMID: 36769410 Free PMC article. Review.
-
Evaluating performance on the Glittre-ADL test in men with long COVID 3 years after a SARS-CoV-2 infection.J Exerc Sci Fit. 2024 Oct;22(4):271-277. doi: 10.1016/j.jesf.2024.03.010. Epub 2024 Mar 29. J Exerc Sci Fit. 2024. PMID: 38601317 Free PMC article.
-
Health-Related Quality of Life and Functional Status of Post-COVID-19 Patients.Int J Environ Res Public Health. 2025 Feb 25;22(3):338. doi: 10.3390/ijerph22030338. Int J Environ Res Public Health. 2025. PMID: 40238313 Free PMC article.
-
European Respiratory Society International Congress 2021: highlights from best-abstract awardees.Breathe (Sheff). 2022 Mar;18(1):210176. doi: 10.1183/20734735.0176-2021. Epub 2022 Apr 5. Breathe (Sheff). 2022. PMID: 36338250 Free PMC article.
-
The Glittre-ADL test in non-hospitalized patients with post-COVID-19 syndrome and its relationship with muscle strength and lung function.Clin Biomech (Bristol). 2022 Dec;100:105797. doi: 10.1016/j.clinbiomech.2022.105797. Epub 2022 Oct 12. Clin Biomech (Bristol). 2022. PMID: 36244099 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous