

The global trends and regional differences in incidence and mortality of hepatitis A from 1990 to 2019 and implications for its prevention
- PMID: 34345993
- PMCID: PMC8514357
- DOI: 10.1007/s12072-021-10232-4
The global trends and regional differences in incidence and mortality of hepatitis A from 1990 to 2019 and implications for its prevention
Abstract
Background and purpose: Despite decades of improved sanitation and hygiene measures and vaccine introduction, hepatitis A has been spread through numerous outbreaks globally. We used data from the Global Burden of Disease (GBD) study to quantify hepatitis A burden at the global, regional and national levels.
Methods: Annual incident cases, deaths, age-standardized incidence rates (ASIRs), and age-standardized mortality rates (ASMRs) of hepatitis A between 1990 and 2019 were derived from the GBD study 2019. Percentage changes of cases and deaths, and estimated annual percentage changes (EAPCs) of ASIRs and ASMRs were calculated to quantify their temporal trends.
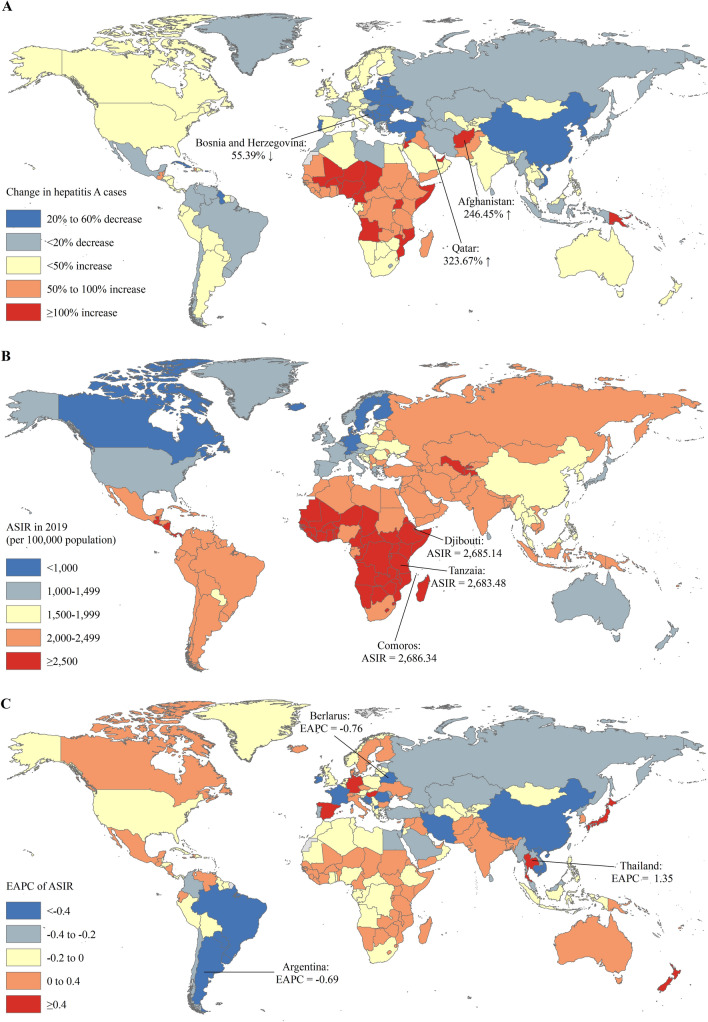
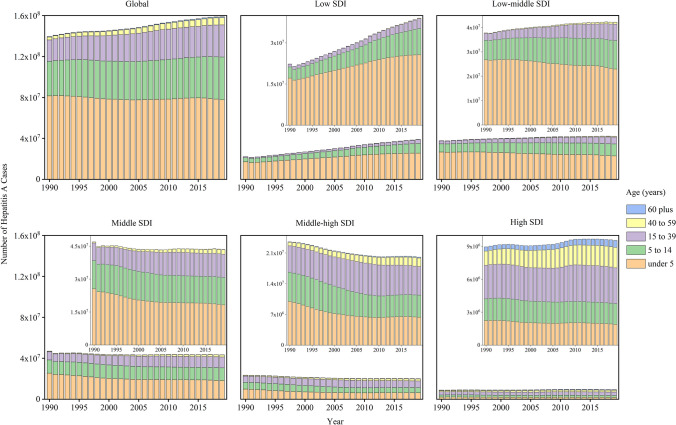
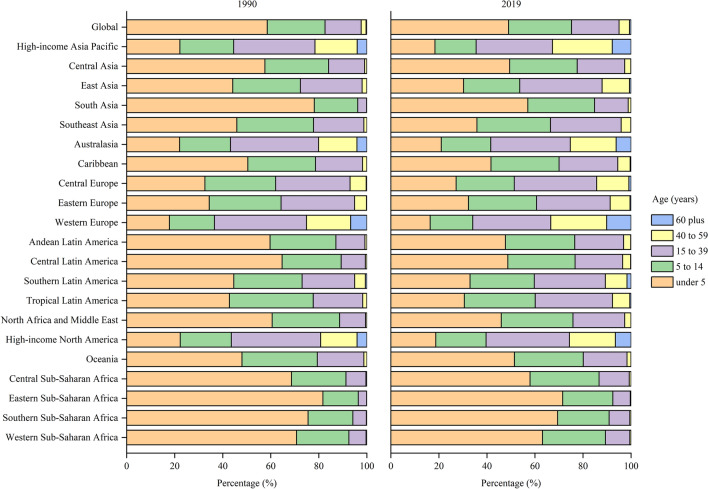
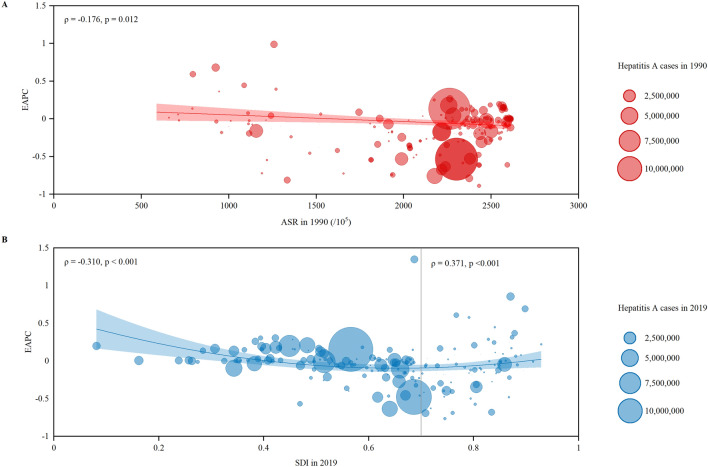
Results: Global hepatitis A incident cases increased by 13.90% from 139.54 million in 1990 to 158.94 million in 2019. ASIR of hepatitis A remained stable (EAPC = 0.00, 95% CI -0.01 to 0.01), whereas ASMR decreased (EAPC = -4.63, 95% CI -4.94 to -4.32) between 1990 and 2019. ASIR increased in low (EAPC = 0.09, 95% CI 0.04 to 0.14) and low-middle (EAPC = 0.04, 95% CI 0.03 to 0.06) socio-demographic index (SDI) regions. For GBD regions, the most significant increases of ASIR were detected in high-income Asia Pacific (EAPC = 0.53, 95% CI 0.41 to 0.66), Oceania (EAPC = 0.31, 95% CI 0.25 to 0.36), and Australasia (EAPC = 0.28, 95% CI 0.13 to 0.44). EAPC of ASIR was positively associated with SDI value in countries and territories with SDI value ≥ 0.7 (ρ = -0.310, p < 0.001).
Conclusion: There is an unfavorable trend that hepatitis A is still pending in hyperendemic regions and is emerging in low endemic regions. These highlight the need of targeted and specific strategies to eliminate hepatitis A, such as sanitation measures and a comprehensive plan for surveillance and vaccination against hepatitis A.
Keywords: Age-standardized incidence rate; Age-standardized mortality rate; Global burden of disease; Hepatitis A; Prevention; Trend.
© 2021. The Author(s).
Conflict of interest statement
Guiying Cao, Wenzhan Jing, Jue Liu, Min Liu declare that they have no conflict of interest.
Figures

References
-
- WHO WHO position paper on hepatitis A vaccines. Weekly Epidemiol Record. 2012;87(28-29):261–276.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
