

Activity detection and classification from wristband accelerometer data collected on people with type 1 diabetes in free-living conditions
- PMID: 34346318
- PMCID: PMC8577986
- DOI: 10.1016/j.compbiomed.2021.104633
Activity detection and classification from wristband accelerometer data collected on people with type 1 diabetes in free-living conditions
Abstract
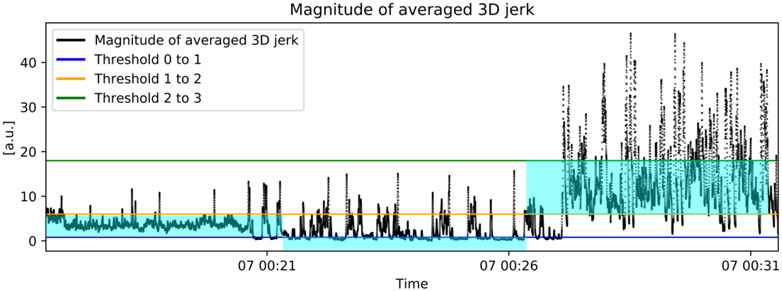
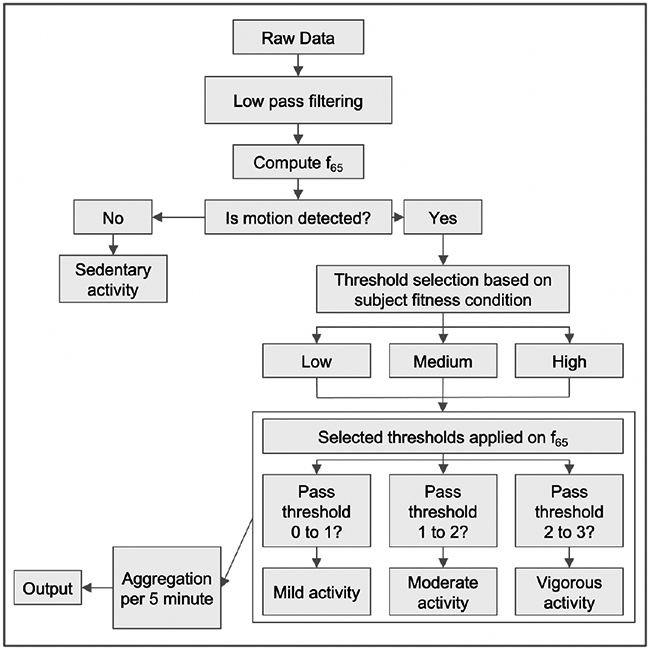
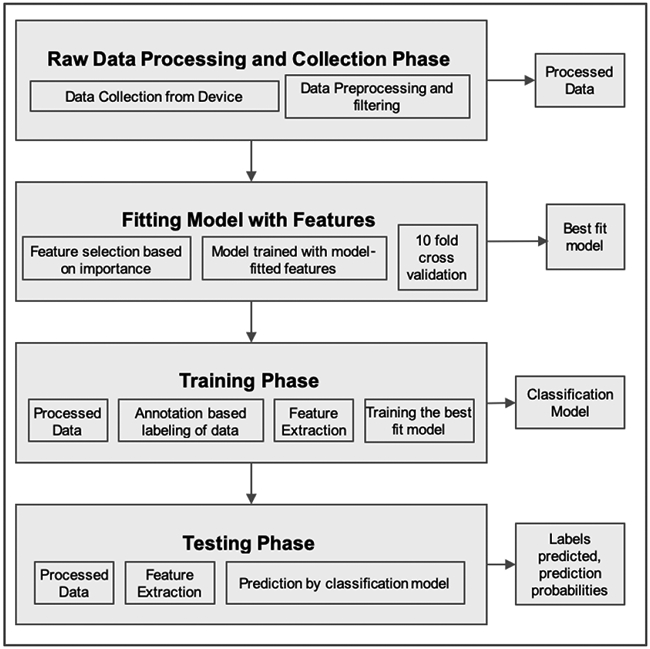
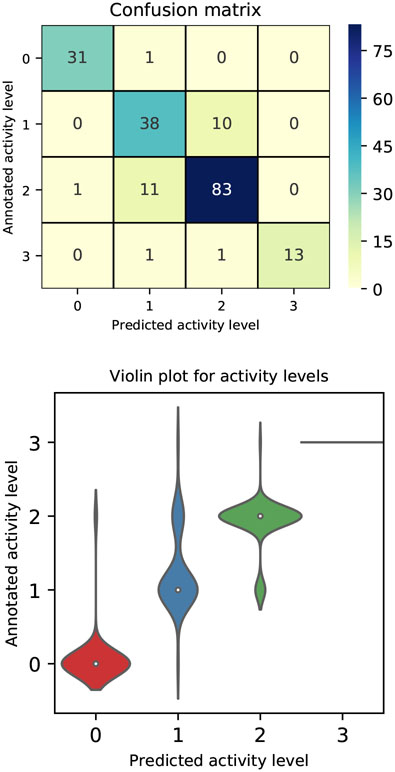
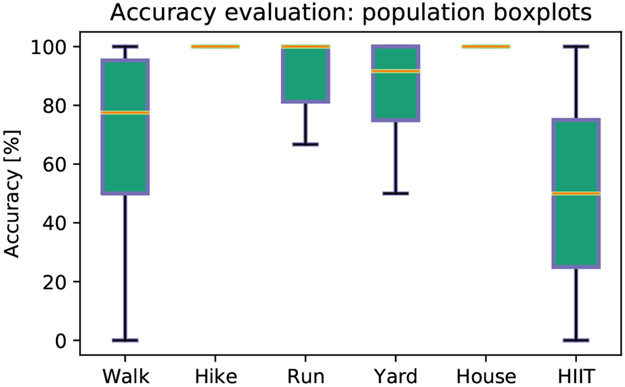
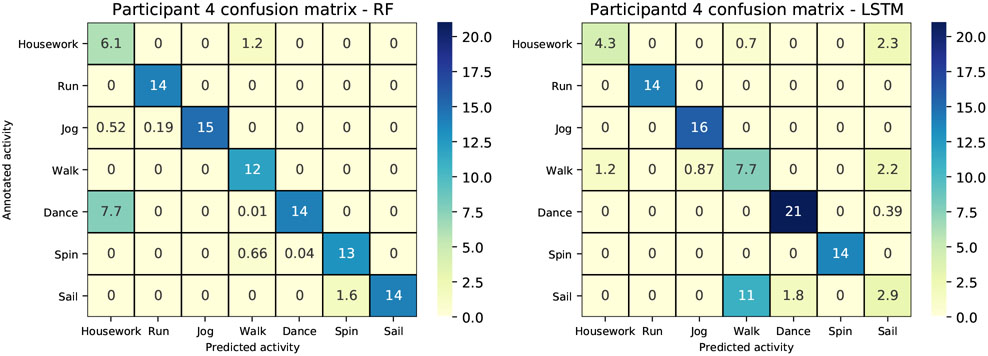
This paper introduces methods to estimate aspects of physical activity and sedentary behavior from three-axis accelerometer data collected with a wrist-worn device at a sampling rate of 32 [Hz] on adults with type 1 diabetes (T1D) in free-living conditions. In particular, we present two methods able to detect and grade activity based on its intensity and individual fitness as sedentary, mild, moderate or vigorous, and a method that performs activity classification in a supervised learning framework to predict specific user behaviors. Population results for activity level grading show multi-class average accuracy of 99.99%, precision of 98.0 ± 2.2%, recall of 97.9 ± 3.5% and F1 score of 0.9 ± 0.0. As for the specific behavior prediction, our best performing classifier, gave population multi-class average accuracy of 92.43 ± 10.32%, precision of 92.94 ± 9.80%, recall of 92.20 ± 10.16% and F1 score of 92.56 ± 9.94%. Our investigation showed that physical activity and sedentary behavior can be detected, graded and classified with good accuracy and precision from three-axial accelerometer data collected in free-living conditions on people with T1D. This is particularly significant in the context of automated glucose control systems for diabetes, in that the methods we propose have the potential to inform changes in treatment parameters in response to the intensity of physical activity, allowing patients to meet their glycemic targets.
Keywords: Artificial pancreas; Automated insulin delivery; Free-living conditions; Physical activity; Supervised learning; Type 1 diabetes mellitus; Wearable devices; Wrist-worn accelerometer.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest declaration
Dr. Cescon serves on the advisory board for Diatech Diabetes, Inc.
Dr. Pinsker reports receiving grant support, provided to his institution, and consulting fees and speaker fees from Tandem Diabetes Care; grant support, provided to his institution, and advisory board fees from Medtronic; grant support, provided to his institution, and consulting fees from Eli Lilly; grant support and supplies, provided to his institution, from Insulet; and supplies, provided to his institution, from Dexcom.
Dr. Kudva reports product support from Dexcom, Roche Diabetes and Tandem.
Dr. Doyle reports equity, licensed IP and is a member of the Scientific Advisory Board of Mode AGC.
Dr. Dassau reports receiving grants from JDRF, NIH, and Helmsley Charitable Trust, personal fees from Roche and Eli Lilly, patents on artificial pancreas technology, and product support from Dexcom, Insulet, Tandem, and Roche. Dr. Dassau is currently an employee and shareholder of Eli Lilly and Company. The work presented in this manuscript was performed as part of his academic appointment and is independent of his employment with Eli Lilly and Company.
No conflicts of interest relevant to this project are reported for the rest of the authors.
Figures
References
-
- Americ. Diabetes Assoc., “Lifestyle management: Standards of medical care in diabetes–2018,” Diabetes Care, vol. 41, no. Supplement 1, pp. S38–S50, 2018. - PubMed
-
- Riddell M, Gallen I, Smart C, Taplin C, Adolfsson P, Lumb A, Kowalski A, Rabasa-Lhoret R, McCrimmon R, Hume C, Annan F, Fournier P, Graham C, Bode B, Galassetti P, Jones T, San Millan I, Heise T, Peters A, Petz A, and Laffel L, “Exercise management in type 1 diabetes: a consensus statement,” Lancet Diab. Endocrinol, vol. 5, pp. 377–390, 2017. - PubMed
-
- Pinsker J, Kraus A, Gianferante D, Schoenberg B, Singh S, Ortiz H, Dassau E, and Kerr D, “Techniques for exercise preparation and management in adults with type 1 diabetes,” Can. J. Diab, vol. 40, no. 6, pp. 503–508, 2016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
