

Evaluation of the INDICAID COVID-19 Rapid Antigen Test in Symptomatic Populations and Asymptomatic Community Testing
- PMID: 34346748
- PMCID: PMC8552729
- DOI: 10.1128/Spectrum.00342-21
Evaluation of the INDICAID COVID-19 Rapid Antigen Test in Symptomatic Populations and Asymptomatic Community Testing
Abstract
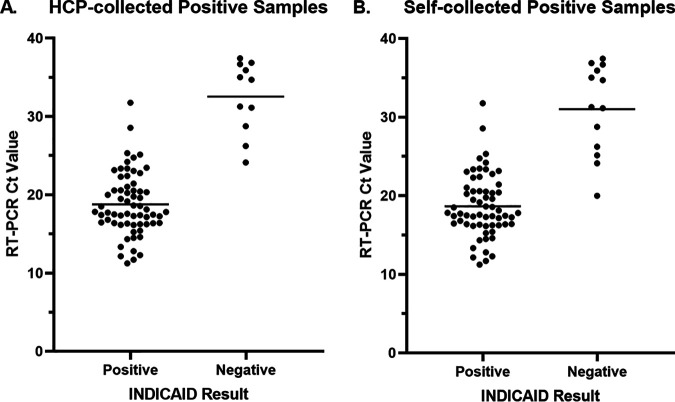
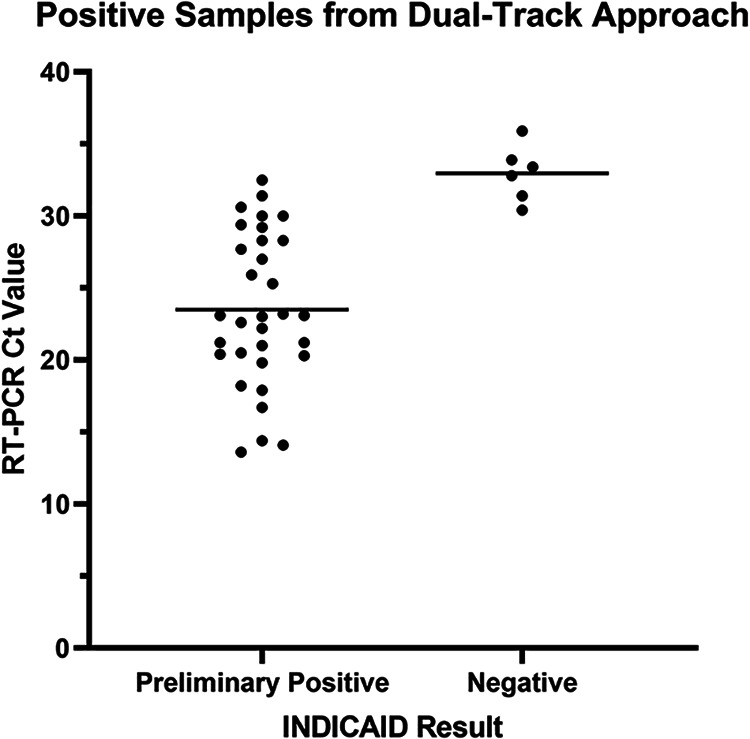
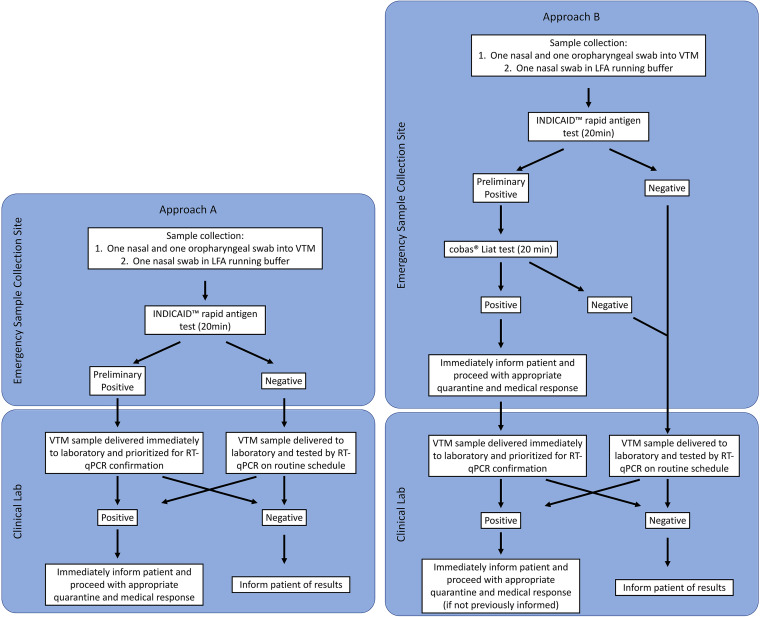
As the COVID-19 pandemic progresses, there is an increasing need for rapid, accessible assays for SARS-CoV-2 detection. We present a clinical evaluation and real-world implementation of the INDICAID COVID-19 rapid antigen test (INDICAID rapid test). A multisite clinical evaluation of the INDICAID rapid test using prospectively collected nasal (bilateral anterior) swab samples from symptomatic subjects was performed. The INDICAID rapid test demonstrated a positive percent agreement (PPA) and negative percent agreement (NPA) of 85.3% (95% confidence interval [95% CI], 75.6% to 91.6%) and 94.9% (95% CI, 91.6% to 96.9%), respectively, compared to laboratory-based reverse transcriptase PCR (RT-PCR) using nasal specimens. The INDICAID rapid test was then implemented at COVID-19 outbreak screening centers in Hong Kong as part of a testing algorithm (termed "dual-track") to screen asymptomatic individuals for prioritization for confirmatory RT-PCR testing. In one approach, preliminary positive INDICAID rapid test results triggered expedited processing for laboratory-based RT-PCR, reducing the average time to confirmatory result from 10.85 h to 7.0 h. In a second approach, preliminary positive results triggered subsequent testing with an onsite rapid RT-PCR, reducing the average time to confirmatory result to 0.84 h. In 22,994 asymptomatic patients, the INDICAID rapid test demonstrated a PPA of 84.2% (95% CI, 69.6% to 92.6%) and an NPA of 99.9% (95% CI, 99.9% to 100%) compared to laboratory-based RT-PCR using combined nasal/oropharyngeal specimens. The INDICAID rapid test has excellent performance compared to laboratory-based RT-PCR testing and, when used in tandem with RT-PCR, reduces the time to confirmatory positive result. IMPORTANCE Laboratory-based RT-PCR, the current gold standard for COVID-19 testing, can require a turnaround time of 24 to 48 h from sample collection to result. The delayed time to result limits the effectiveness of centralized RT-PCR testing to reduce transmission and stem potential outbreaks. To address this, we conducted a thorough evaluation of the INDICAID COVID-19 rapid antigen test, a 20-minute rapid antigen test, in both symptomatic and asymptomatic populations. The INDICAID rapid test demonstrated high sensitivity and specificity with RT-PCR as the comparator method. A dual-track testing algorithm was also evaluated utilizing the INDICAID rapid test to screen for preliminary positive patients, whose samples were then prioritized for RT-PCR testing. The dual-track method demonstrated significant improvements in expediting the reporting of positive RT-PCR test results compared to standard RT-PCR testing without prioritization, offering an improved strategy for community testing and controlling SARS-CoV-2 outbreaks.
Keywords: COVID-19; Hong Kong; SARS-CoV-2; USA; antigen; asymptomatic screening; rapid.
Figures
References
-
- FDA. 2020. Policy for coronavirus disease-2019 tests during the public health emergency (revised): immediately in effect guidance for clinical laboratories, commercial manufacturers, and food and drug administration staff.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
