

Blood DNA Methylation and Incident Coronary Heart Disease: Evidence From the Strong Heart Study
- PMID: 34347013
- PMCID: PMC8340006
- DOI: 10.1001/jamacardio.2021.2704
Blood DNA Methylation and Incident Coronary Heart Disease: Evidence From the Strong Heart Study
Abstract
Importance: American Indian communities experience a high burden of coronary heart disease (CHD). Strategies are needed to identify individuals at risk and implement preventive interventions.
Objective: To investigate the association of blood DNA methylation (DNAm) with incident CHD using a large number of methylation sites (cytosine-phosphate-guanine [CpG]) in a single model.
Design, setting, and participants: This prospective study, including a discovery cohort (the Strong Heart Study [SHS]) and 4 additional cohorts (the Women's Health Initiative [WHI], the Framingham Heart Study [FHS], the Atherosclerosis Risk in Communities Study ([ARIC]-Black, and ARIC-White), evaluated 12 American Indian communities in 4 US states; African American women, Hispanic women, and White women throughout the US; White men and White women from Massachusetts; and Black men and women and White men and women from 4 US communities. A total of 2321 men and women (mean [SD] follow-up, 19.1 [9.2] years) were included in the SHS, 1874 women (mean [SD] follow-up, 15.8 [5.9] years) in the WHI, 2128 men and women (mean [SD] follow-up, 7.7 [1.8] years) in the FHS, 2114 men and women (mean [SD] follow-up, 20.9 [7.2] years) in the ARIC-Black, and 931 men and women (mean [SD] follow-up, 20.9 [7.2] years) in the ARIC-White. Data were collected from May 1989 to December 2018 and analyzed from February 2019 to May 2021.
Exposure: Blood DNA methylation.
Main outcome and measure: Using a high-dimensional time-to-event elastic-net model for the association of 407 224 CpG sites with incident CHD in the SHS (749 events), this study selected the differentially methylated CpG positions (DMPs) selected in the SHS and evaluated them in the WHI (531 events), FHS (143 events), ARIC-Black (350 events), and ARIC-White (121 events) cohorts.
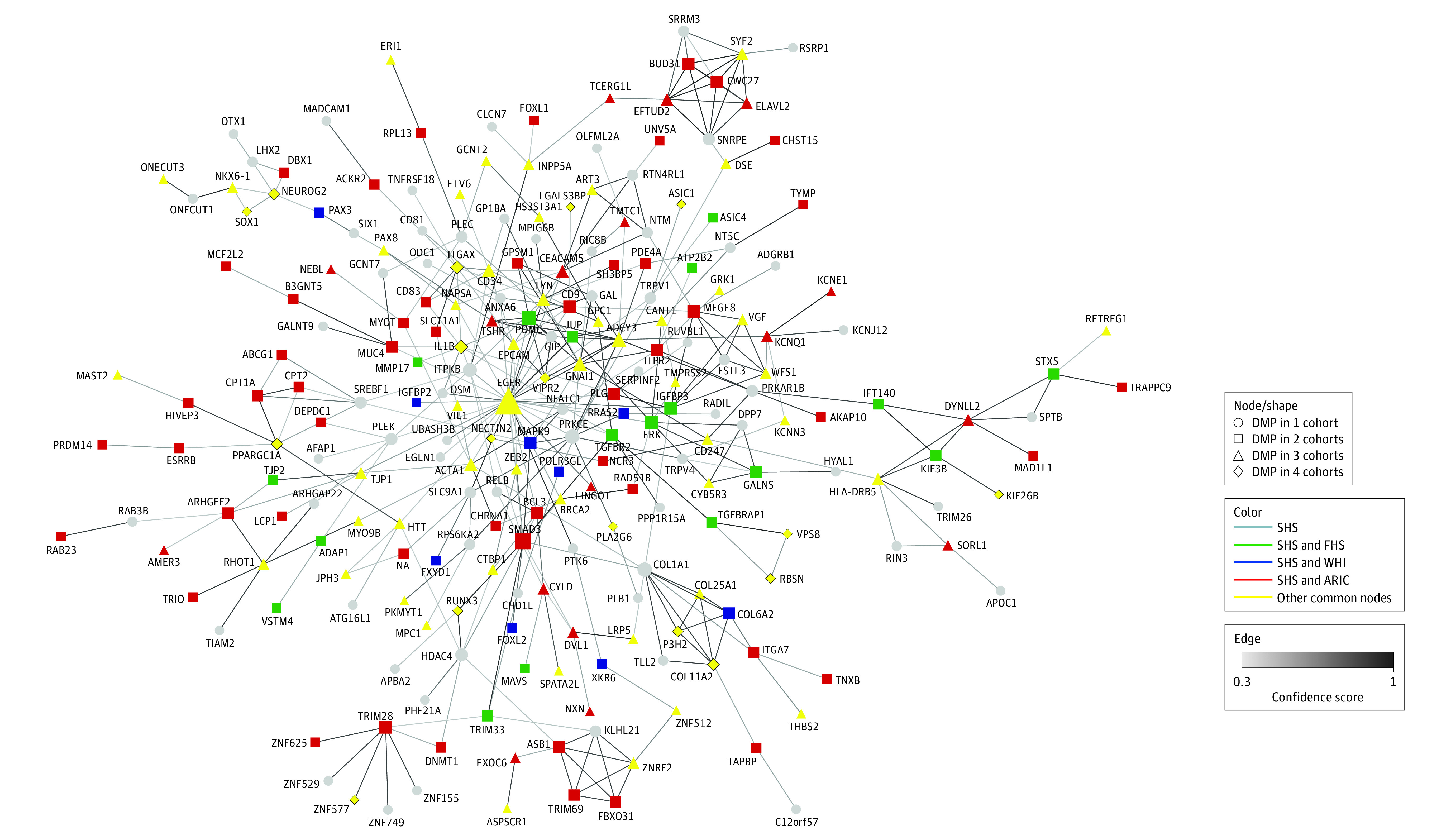
Results: The median (IQR) age of participants in SHS was 55 (49-62) years, and 1359 participants (58.6%) were women. Elastic-net models selected 505 DMPs associated with incident CHD in the SHS beyond established risk factors, center, blood cell counts, and genetic principal components. Among those DMPs, 33 were commonly selected in 3 or 4 of the other cohorts and the pooled hazard ratios from the standard Cox models were significant at P < .05 for 10 of the DMPs. For example, the hazard ratio (95% CI) for CHD comparing the 90th and 10th percentiles of differentially methylated CpGs was 0.86 (0.78-0.95) for cg16604233 (tagged to COL11A2) and 1.23 (1.08-1.39) for cg09926486 (tagged to FRMD5). Some of the DMPs were consistent in the direction of the association; others showed associations in opposite directions across cohorts. Untargeted independent elastic-net models of CHD showed distinct DMPs, genes, and network of genes in the 5 cohorts.
Conclusions and relevance: In this multi-cohort study, blood-based DNAm findings supported an association between a complex blood epigenomic signature and CHD that was largely different across populations.
Conflict of interest statement
Figures
References
-
- Breathett K, Sims M, Gross M, et al. ; American Heart Association Council on Epidemiology and Prevention; Council on Quality of Care and Outcomes Research; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Lifestyle and Cardiometabolic Health . Cardiovascular health in American Indians and Alaska Natives: a scientific statement from the American Heart Association. Circulation. 2020;141(25):e948-e959. doi: 10.1161/CIR.0000000000000773 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201600001C/HL/NHLBI NIH HHS/United States
- R01 ES025216/ES/NIEHS NIH HHS/United States
- R01 ES021367/ES/NIEHS NIH HHS/United States
- P42 ES010349/ES/NIEHS NIH HHS/United States
- R01 HL109319/HL/NHLBI NIH HHS/United States
- R01 HL109315/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- R01 HL109284/HL/NHLBI NIH HHS/United States
- N01HC25195/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- R01 HL109301/HL/NHLBI NIH HHS/United States
- P30 ES009089/ES/NIEHS NIH HHS/United States
- R25 ES025505/ES/NIEHS NIH HHS/United States
- HHSN268201600003C/HL/NHLBI NIH HHS/United States
- R01 NS087541/NS/NINDS NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- R01 HL109282/HL/NHLBI NIH HHS/United States
- HHSN268201600002C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201600004C/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
- R01 HL090863/HL/NHLBI NIH HHS/United States
- HHSN268201600018C/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous
