

Congenital anomalies and genetic disorders in neonates and infants: a single-center observational cohort study
- PMID: 34347148
- PMCID: PMC8760213
- DOI: 10.1007/s00431-021-04213-w
Congenital anomalies and genetic disorders in neonates and infants: a single-center observational cohort study
Abstract
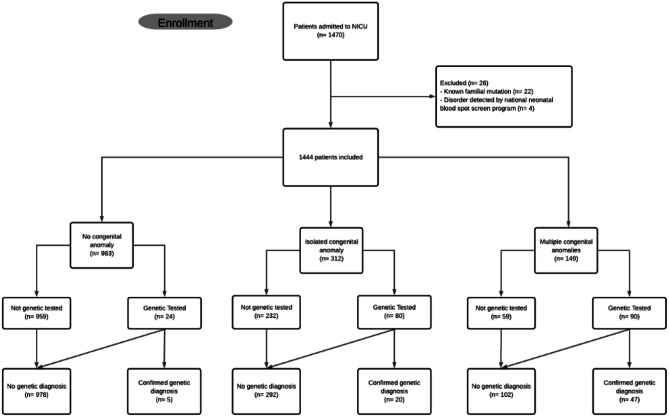
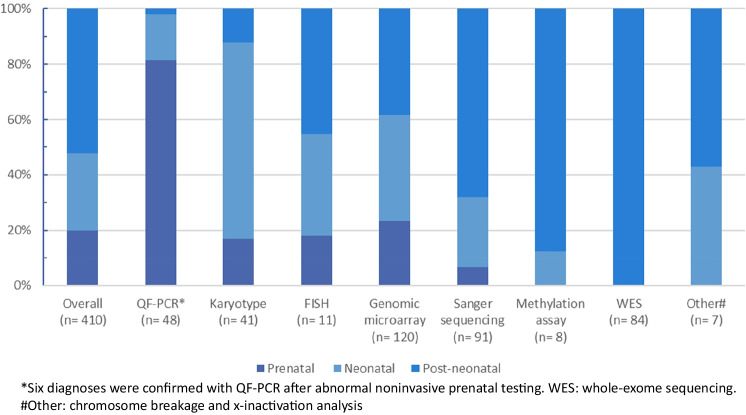
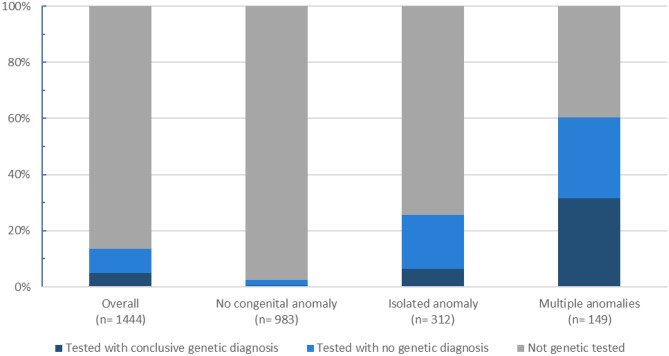
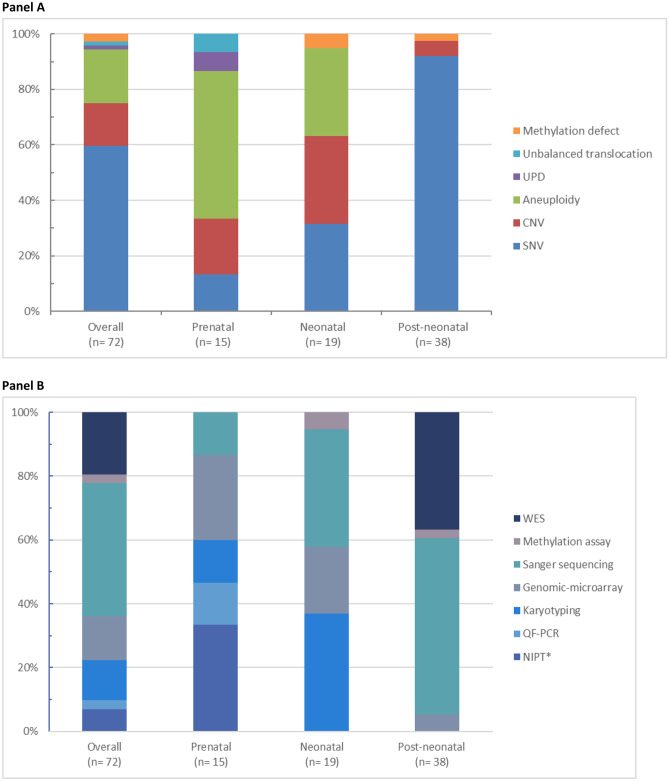
Neonates with genetic disorders or congenital anomalies (CA) contribute considerably to morbidity and mortality in neonatal intensive care units (NICUs). The objective of this study is to study the prevalence of genetic disorders in an academic level IV NICU. We retrospective collected and analyzed both clinical and genetic data of all 1444 infants admitted to the NICU of the Radboudumc (October 2013 to October 2015). Data were collected until infants reached at least 2 years of age. A total of 13% (194/1444) of the patients were genetically tested, and 32% (461/1444) had a CA. A total of 37% (72/194) had a laboratory-confirmed genetic diagnosis. In 53%, the diagnosis was made post-neonatally (median age = 209 days) using assays including exome sequencing. Exactly 63% (291/461) of the patients with CA, however, never received genetic testing, despite being clinically similar those who did.Conclusions: Genetic disorders were suspected in 13% of the cohort, but only confirmed in 5%. Most received their genetic diagnosis in the post-neonatal period. Extrapolation of the diagnostic yield suggests that up to 6% of our cohort may have remained genetically undiagnosed. Our data show the need to improve genetic care in the NICU for more inclusive, earlier, and faster genetic diagnosis to enable tailored management. What is Known: • Genetic disorders are suspected in many neonates but only genetically confirmed in a minority. • The presence of a genetic disorder can be easily missed and will often lead to a diagnostic odyssey requiring extensive evaluations, both clinically and genetically. What is New: • Different aspects of the clinical features and uptake of genetic test in a NICU cohort. • The need to improve genetic care in the NICU for more inclusive, earlier, and faster genetic diagnosis to enable tailored management.
Keywords: Diagnostic yield; Genetic diagnosis; NICU; Neonatal intensive care unit; Neonates.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Swaggart KA, Swarr DT, Tolusso LK, He H, Dawson DB, Suhrie KR (2019) Making a genetic diagnosis in a level IV neonatal intensive care unit population: Who, when, how, and at what cost? J Pediatr 213:211–7 e4 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
