

Clinical and biological clusters of sepsis patients using hierarchical clustering
- PMID: 34347776
- PMCID: PMC8336799
- DOI: 10.1371/journal.pone.0252793
Clinical and biological clusters of sepsis patients using hierarchical clustering
Abstract
Background: Heterogeneity in sepsis expression is multidimensional, including highly disparate data such as the underlying disorders, infection source, causative micro-organismsand organ failures. The aim of the study is to identify clusters of patients based on clinical and biological characteristic available at patients' admission.
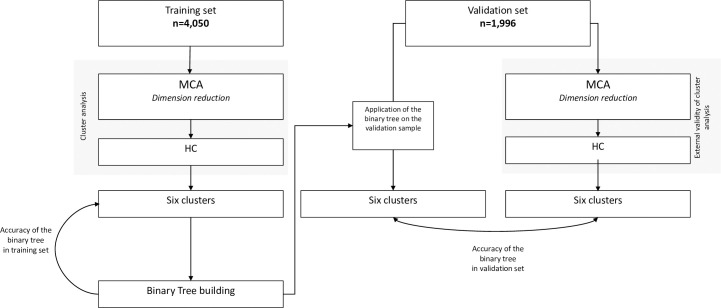
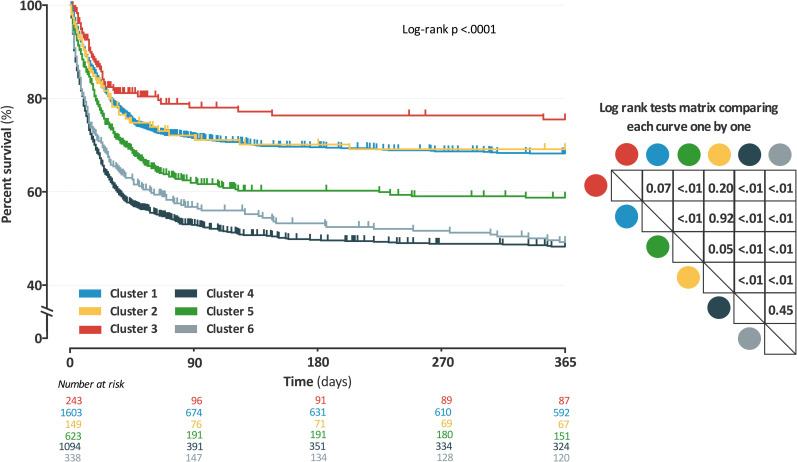
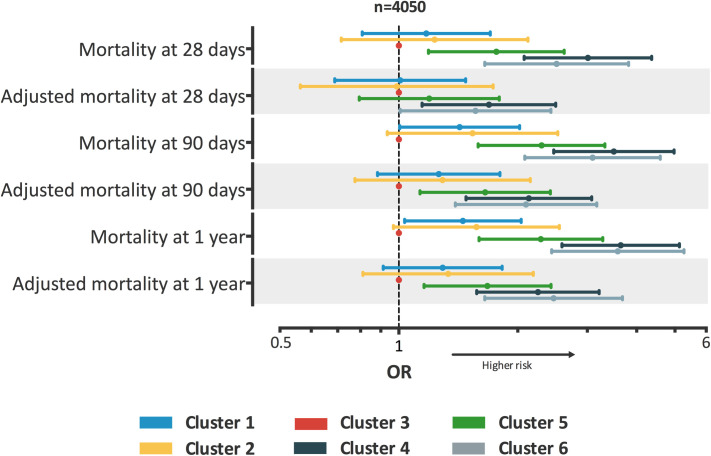
Methods: All patients included in a national prospective multicenter ICU cohort OUTCOMEREA and admitted for sepsis or septic shock (Sepsis 3.0 definition) were retrospectively analyzed. A hierarchical clustering was performed in a training set of patients to build clusters based on a comprehensive set of clinical and biological characteristics available at ICU admission. Clusters were described, and the 28-day, 90-day, and one-year mortality were compared with log-rank rates. Risks of mortality were also compared after adjustment on SOFA score and year of ICU admission.
Results: Of the 6,046 patients with sepsis in the cohort, 4,050 (67%) were randomly allocated to the training set. Six distinct clusters were identified: young patients without any comorbidities, admitted in ICU for community-acquired pneumonia (n = 1,603 (40%)); young patients without any comorbidities, admitted in ICU for meningitis or encephalitis (n = 149 (4%)); elderly patients with COPD, admitted in ICU for bronchial infection with few organ failures (n = 243 (6%)); elderly patients, with several comorbidities and organ failures (n = 1,094 (27%)); patients admitted after surgery, with a nosocomial infection (n = 623 (15%)); young patients with immunosuppressive conditions (e.g., AIDS, chronic steroid therapy or hematological malignancy) (n = 338 (8%)). Clusters differed significantly in early or late mortality (p < .001), even after adjustment on severity of organ dysfunctions (SOFA) and year of ICU admission.
Conclusions: Clinical and biological features commonly available at ICU admission of patients with sepsis or septic shock enabled to set up six clusters of patients, with very distinct outcomes. Considering these clusters may improve the care management and the homogeneity of patients in future studies.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Shankar-Hari M, Phillips GS, Levy ML, Seymour CW, Liu VX, et al. (2016) Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 315: 775–787. doi: 10.1001/jama.2016.0289 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
