

Hierarchical clustering by patient-reported pain distribution alone identifies distinct chronic pain subgroups differing by pain intensity, quality, and clinical outcomes
- PMID: 34347793
- PMCID: PMC8336800
- DOI: 10.1371/journal.pone.0254862
Hierarchical clustering by patient-reported pain distribution alone identifies distinct chronic pain subgroups differing by pain intensity, quality, and clinical outcomes
Abstract
Background: In clinical practice, the bodily distribution of chronic pain is often used in conjunction with other signs and symptoms to support a diagnosis or treatment plan. For example, the diagnosis of fibromyalgia involves tallying the areas of pain that a patient reports using a drawn body map. It remains unclear whether patterns of pain distribution independently inform aspects of the pain experience and influence patient outcomes. The objective of the current study was to evaluate the clinical relevance of patterns of pain distribution using an algorithmic approach agnostic to diagnosis or patient-reported facets of the pain experience.
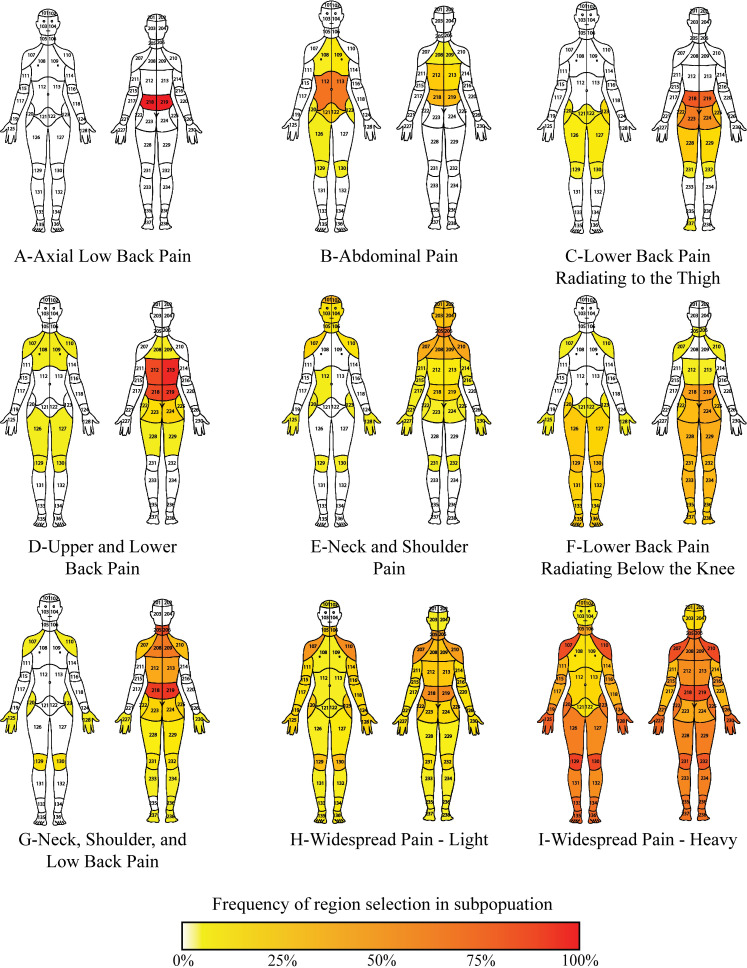
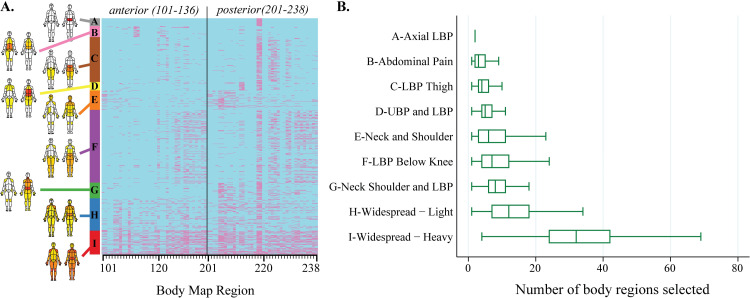
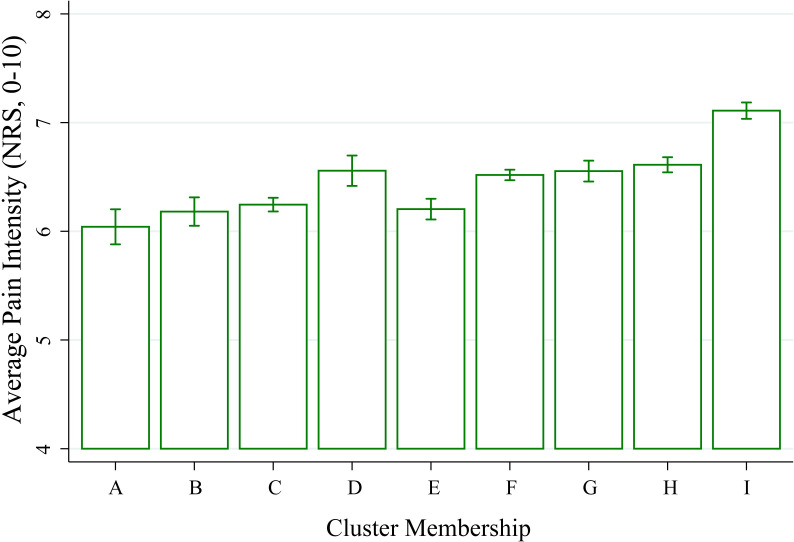
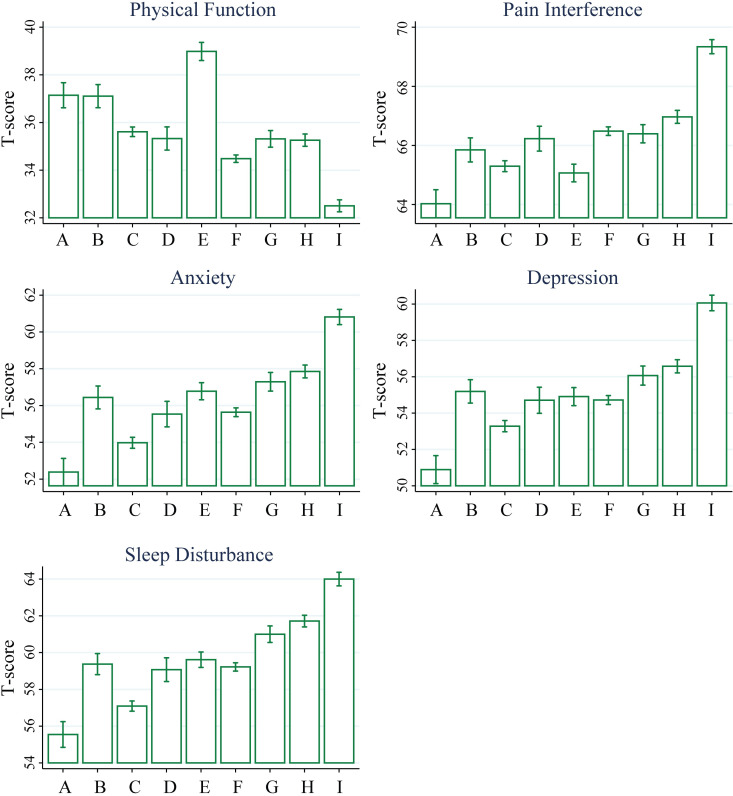
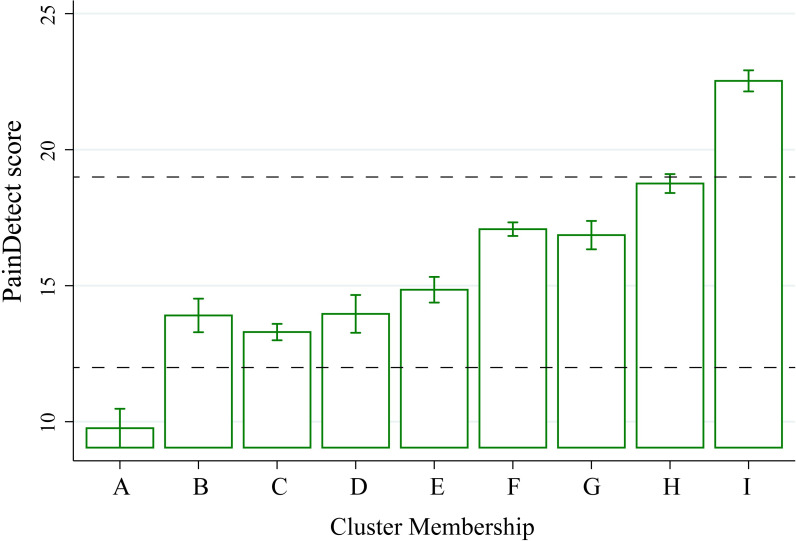
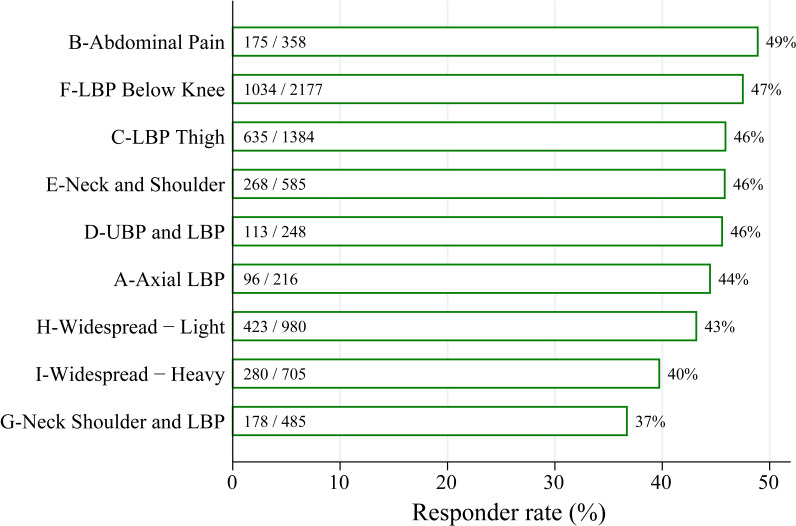
Methods and findings: A large cohort of patients (N = 21,658) completed pain body maps and a multi-dimensional pain assessment. Using hierarchical clustering of patients by body map selection alone, nine distinct subgroups emerged with different patterns of body region selection. Clinician review of cluster body maps recapitulated some clinically-relevant patterns of pain distribution, such as low back pain with radiation below the knee and widespread pain, as well as some unique patterns. Demographic and medical characteristics, pain intensity, pain impact, and neuropathic pain quality all varied significantly across cluster subgroups. Multivariate modeling demonstrated that cluster membership independently predicted pain intensity and neuropathic pain quality. In a subset of patients who completed 3-month follow-up questionnaires (N = 7,138), cluster membership independently predicted the likelihood of improvement in pain, physical function, and a positive overall impression of change related to multidisciplinary pain care.
Conclusions: This study reports a novel method of grouping patients by pain distribution using an algorithmic approach. Pain distribution subgroup was significantly associated with differences in pain intensity, impact, and clinically relevant outcomes. In the future, algorithmic clustering by pain distribution may be an important facet in chronic pain biosignatures developed for the personalization of pain management.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Korwisi B, Hay G, Attal N, Aziz Q, Bennett MI, Benoliel R, et al. Classification algorithm for the International Classification of Diseases-11 chronic pain classification: development and results from a preliminary pilot evaluation. Pain. 2021. Epub 2021/01/26. doi: 10.1097/j.pain.0000000000002208 . - DOI - PubMed
-
- Kent ML, Tighe PJ, Belfer I, Brennan TJ, Bruehl S, Brummett CM, et al. The ACTTION-APS-AAPM Pain Taxonomy (AAAPT) Multidimensional Approach to Classifying Acute Pain Conditions. J Pain. 2017;18(5):479–89. Epub 2017/05/13. doi: 10.1016/j.jpain.2017.02.421 ; PubMed Central PMCID: PMC7323793. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
