

Evaluation of Immune Response and Disease Status in Systemic Lupus Erythematosus Patients Following SARS-CoV-2 Vaccination
- PMID: 34347939
- PMCID: PMC8426963
- DOI: 10.1002/art.41937
Evaluation of Immune Response and Disease Status in Systemic Lupus Erythematosus Patients Following SARS-CoV-2 Vaccination
Abstract
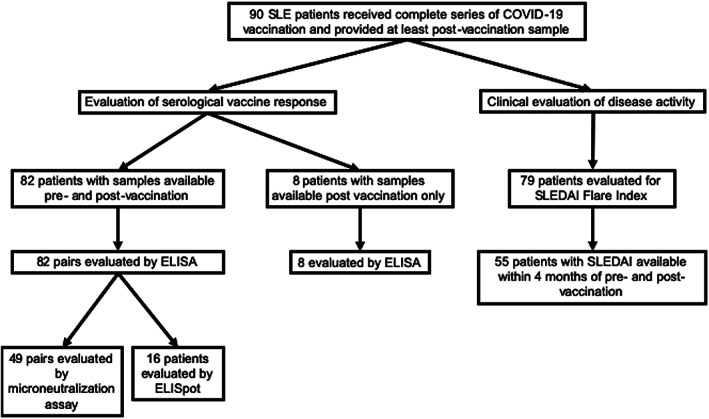
Objective: To evaluate seroreactivity and disease flares after COVID-19 vaccination in a multiethnic/multiracial cohort of patients with systemic lupus erythematosus (SLE).
Methods: Ninety SLE patients and 20 healthy controls receiving a complete COVID-19 vaccine regimen were included. IgG seroreactivity to the SARS-CoV-2 spike receptor-binding domain (RBD) and SARS-CoV-2 microneutralization were used to evaluate B cell responses; interferon-γ (IFNγ) production was measured by enzyme-linked immunospot (ELISpot) assay in order to assess T cell responses. Disease activity was measured by the hybrid SLE Disease Activity Index (SLEDAI), and flares were identified according to the Safety of Estrogens in Lupus Erythematosus National Assessment-SLEDAI flare index.
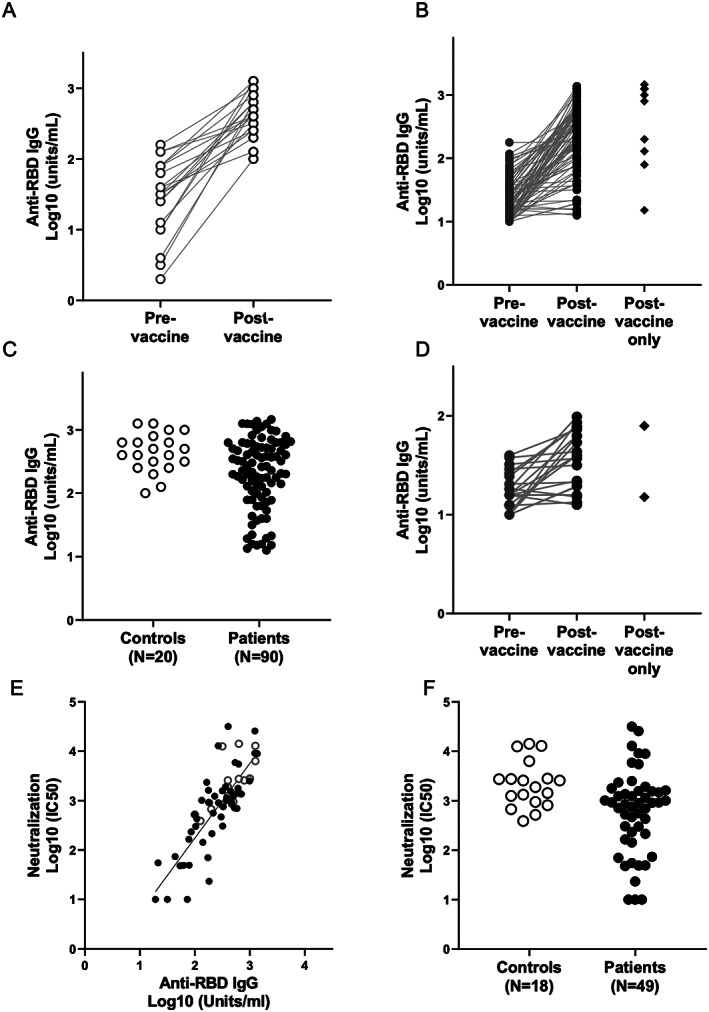
Results: Overall, fully vaccinated SLE patients produced significantly lower IgG antibodies against SARS-CoV-2 spike RBD compared to fully vaccinated controls. Twenty-six SLE patients (28.8%) generated an IgG response below that of the lowest control (<100 units/ml). In logistic regression analyses, the use of any immunosuppressant or prednisone and a normal anti-double-stranded DNA antibody level prior to vaccination were associated with decreased vaccine responses. IgG seroreactivity to the SARS-CoV-2 spike RBD strongly correlated with the SARS-CoV-2 microneutralization titers and correlated with antigen-specific IFNγ production determined by ELISpot. In a subset of patients with poor antibody responses, IFNγ production was similarly diminished. Pre- and postvaccination SLEDAI scores were similar in both groups. Postvaccination flares occurred in 11.4% of patients; 1.3% of these were severe.
Conclusion: In a multiethnic/multiracial study of SLE patients, 29% had a low response to the COVID-19 vaccine which was associated with receiving immunosuppressive therapy. Reassuringly, severe disease flares were rare. While minimal protective levels remain unknown, these data suggest that protocol development is needed to assess the efficacy of booster vaccination.
© 2021, American College of Rheumatology.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
