

Learning from patient safety incidents involving acutely sick adults in hospital assessment units in England and Wales: a mixed methods analysis for quality improvement
- PMID: 34348052
- PMCID: PMC8722780
- DOI: 10.1177/01410768211032589
Learning from patient safety incidents involving acutely sick adults in hospital assessment units in England and Wales: a mixed methods analysis for quality improvement
Abstract
Objective: Six per cent of hospital patients experience a patient safety incident, of which 12% result in severe/fatal outcomes. Acutely sick patients are at heightened risk. Our aim was to identify the most frequently reported incidents in acute medical units and their characteristics.
Design: Retrospective mixed methods methodology: (1) an a priori coding process, applying a multi-axial coding framework to incident reports; and, (2) a thematic interpretative analysis of reports.
Setting: Patient safety incident reports (10 years, 2005-2015) collected from the National Reporting and Learning System, which receives reports from hospitals and other care settings across England and Wales.
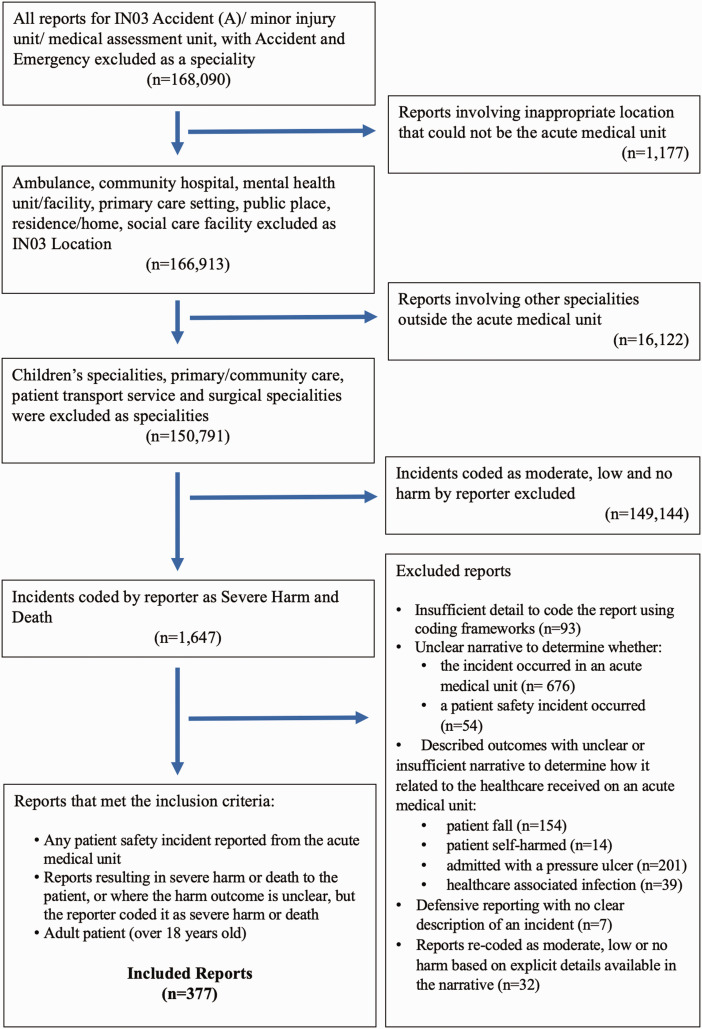
Participants: Reports describing severe harm/death in acute medical unit were identified.
Main outcome measures: Incident type, contributory factors, outcomes and level of harm were identified in the included reports. During thematic analysis, themes and metathemes were synthesised to inform priorities for quality improvement.
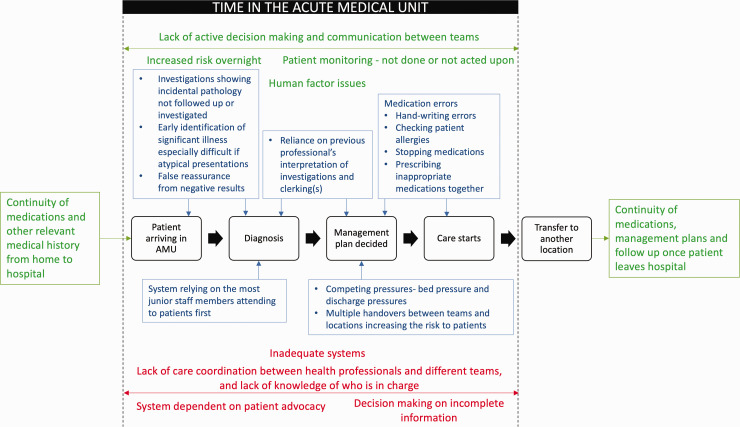
Results: A total of 377 reports of severe harm or death were confirmed. The most common incident types were diagnostic errors (n = 79), medication-related errors (n = 61), and failures monitoring patients (n = 57). Incidents commonly stemmed from lack of active decision-making during patient admissions and communication failures between teams. Patients were at heightened risk of unsafe care during handovers and transfers of care. Metathemes included the necessity of patient self-advocacy and a lack of care coordination.
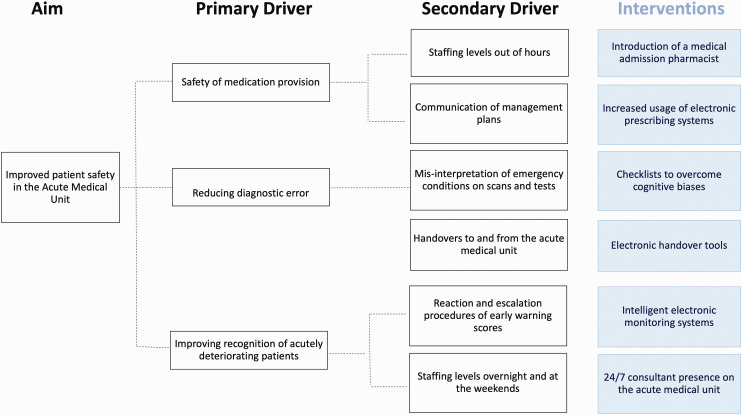
Conclusion: This 10-year national analysis of incident reports provides recommendations to improve patient safety including: introduction of electronic prescribing and monitoring systems; forcing checklists to reduce diagnostic errors; and increased senior presence overnight and at weekends.
Keywords: Clinical; emergency medicine; health service research; medical error/patient safety; medical management; other emergency medicine; other statistics and research methods; quality improvement.
Figures
Similar articles
-
A mixed-methods analysis of patient safety incidents involving opioid substitution treatment with methadone or buprenorphine in community-based care in England and Wales.Addiction. 2020 Nov;115(11):2066-2076. doi: 10.1111/add.15039. Epub 2020 Apr 27. Addiction. 2020. PMID: 32149443
-
Sources of unsafe primary care for older adults: a mixed-methods analysis of patient safety incident reports.Age Ageing. 2017 Sep 1;46(5):833-839. doi: 10.1093/ageing/afx044. Age Ageing. 2017. PMID: 28520904 Free PMC article.
-
Patient Safety Incidents Involving Sick Children in Primary Care in England and Wales: A Mixed Methods Analysis.PLoS Med. 2017 Jan 17;14(1):e1002217. doi: 10.1371/journal.pmed.1002217. eCollection 2017 Jan. PLoS Med. 2017. PMID: 28095408 Free PMC article.
-
A review of medication incidents reported to the National Reporting and Learning System in England and Wales over 6 years (2005-2010).Br J Clin Pharmacol. 2012 Oct;74(4):597-604. doi: 10.1111/j.1365-2125.2011.04166.x. Br J Clin Pharmacol. 2012. PMID: 22188210 Free PMC article. Review.
-
Characterising the nature of primary care patient safety incident reports in the England and Wales National Reporting and Learning System: a mixed-methods agenda-setting study for general practice.Southampton (UK): NIHR Journals Library; 2016 Sep. Southampton (UK): NIHR Journals Library; 2016 Sep. PMID: 27656729 Free Books & Documents. Review.
Cited by
-
Medication-related interventions to improve medication safety and patient outcomes on transition from adult intensive care settings: a systematic review and meta-analysis.BMJ Qual Saf. 2022 Aug;31(8):609-622. doi: 10.1136/bmjqs-2021-013760. Epub 2022 Jan 18. BMJ Qual Saf. 2022. PMID: 35042765 Free PMC article.
-
Student Nurses' Perceptions of the Role of High-Fidelity Simulation in Developing Decision-Making Skills for Clinical Practice: A Qualitative Research Study.SAGE Open Nurs. 2024 May 20;10:23779608241255299. doi: 10.1177/23779608241255299. eCollection 2024 Jan-Dec. SAGE Open Nurs. 2024. PMID: 38770422 Free PMC article.
-
Understanding the scale and nature of avoidable healthcare-associated harm for prisoners in England: protocol for a retrospective cross-sectional study.BMJ Open. 2024 Dec 20;14(12):e085607. doi: 10.1136/bmjopen-2024-085607. BMJ Open. 2024. PMID: 39806709 Free PMC article.
-
Multiple points of system failure underpin continuous subcutaneous infusion safety incidents in palliative care: A mixed methods analysis.Palliat Med. 2025 Jan;39(1):7-21. doi: 10.1177/02692163241287639. Epub 2024 Oct 23. Palliat Med. 2025. PMID: 39444150 Free PMC article.
-
Prioritising health and wellbeing: the hope we cling to in 2021.J R Soc Med. 2021 Dec;114(12):543. doi: 10.1177/01410768211065728. J R Soc Med. 2021. PMID: 34935560 Free PMC article. No abstract available.
References
-
- The Royal College of Physicians of London. Acute Medicine: Organisation and Training for the Next Decade, London: The Royal College of Physicians of London, 2004.
-
- Martin IC, Mason DG, Stewart J, et al. Emergency Admissions: A Journey in the Right Direction?, London, UK: National Confidential Enquiry into Patient Outcome and Death, 2007.
-
- Conway R, O'Riordan D, Silke B. Long-term outcome of an AMAU – a decade's experience. QJM 2013; 107: 7–7. - PubMed
-
- Bangor-Raju D, Mudannayake RS, Subbe CP. Safety in the acute medical unit: the role of severity of illness, structure of communication and staffing. Br J Hosp Med 2015; 76(9): C141--144–C141--144. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
