

Management of proximal femur fractures in the elderly: current concepts and treatment options
- PMID: 34348796
- PMCID: PMC8335457
- DOI: 10.1186/s40001-021-00556-0
Management of proximal femur fractures in the elderly: current concepts and treatment options
Abstract
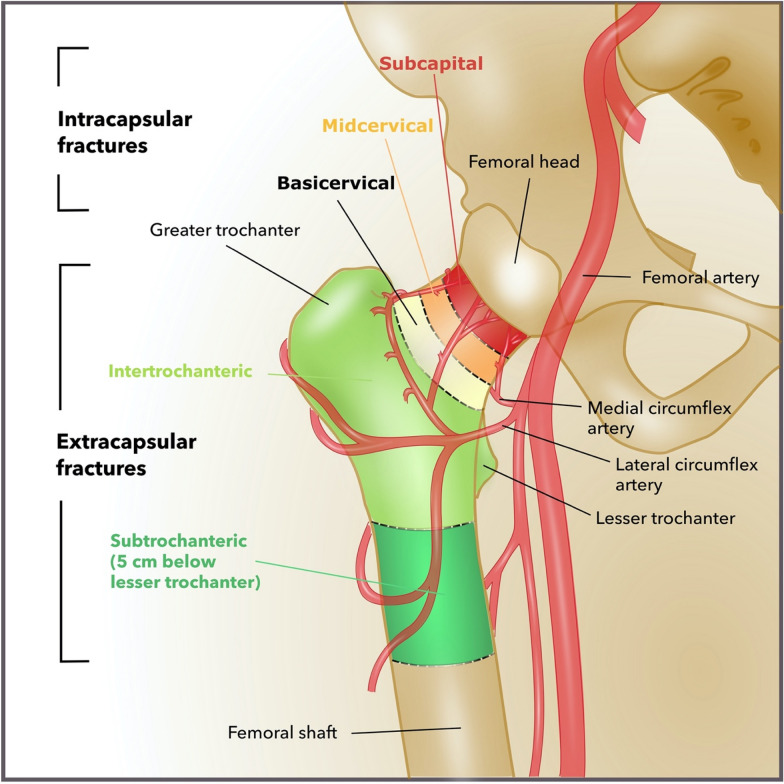
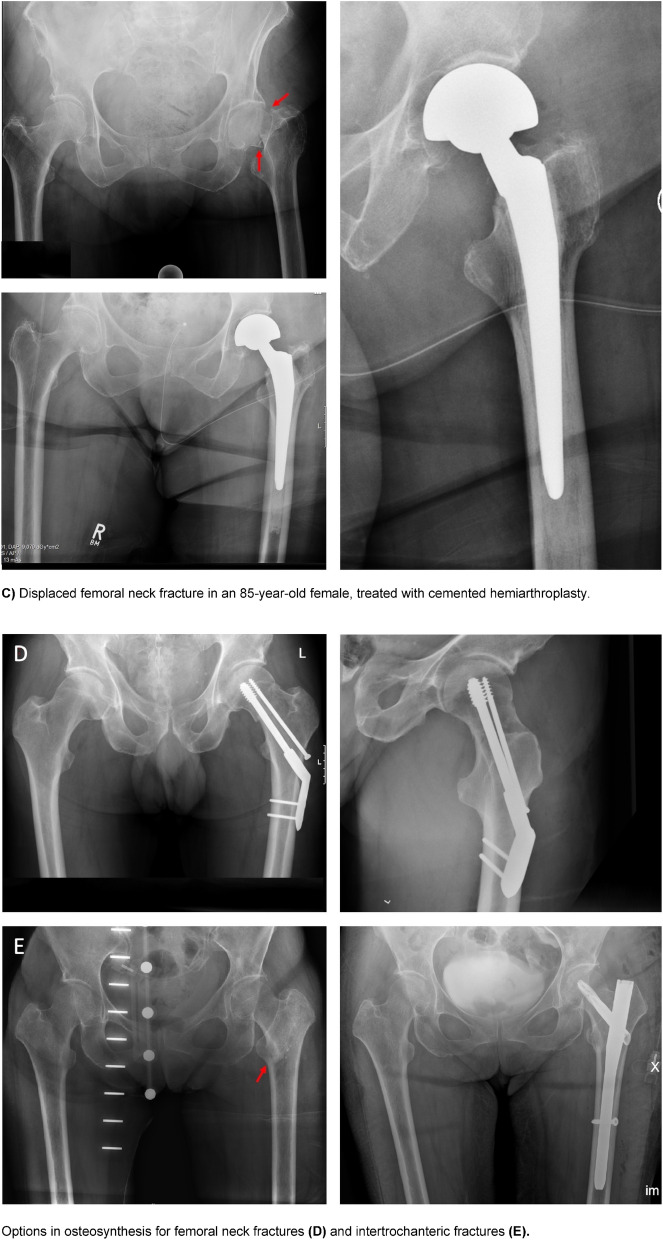
As one of the leading causes of elderly patients' hospitalisation, proximal femur fractures (PFFs) will present an increasing socioeconomic problem in the near future. This is a result of the demographic change that is expressed by the increasing proportion of elderly people in society. Peri-operative management must be handled attentively to avoid complications and decrease mortality rates. To deal with the exceptional needs of the elderly, the development of orthogeriatric centres to support orthogeriatric co-management is mandatory. Adequate pain medication, balanced fluid management, delirium prevention and the operative treatment choice based on comorbidities, individual demands and biological rather than chronological age, all deserve particular attention to improve patients' outcomes. The operative management of intertrochanteric and subtrochanteric fractures favours intramedullary nailing. For femoral neck fractures, the Garden classification is used to differentiate between non-displaced and displaced fractures. Osteosynthesis is suitable for biologically young patients with non-dislocated fractures, whereas total hip arthroplasty and hemiarthroplasty are the main options for biologically old patients and displaced fractures. In bedridden patients, osteosynthesis might be an option to establish transferability from bed to chair and the restroom. Postoperatively, the patients benefit from early mobilisation and early geriatric care. During the COVID-19 pandemic, prolonged time until surgery and thus an increased rate of complications took a toll on frail patients with PFFs. This review aims to offer surgical guidelines for the treatment of PFFs in the elderly with a focus on pitfalls and challenges particularly relevant to frail patients.
Keywords: Delirium prevention; Frailty; Garden classification; Surgical management.
© 2021. The Author(s).
Conflict of interest statement
Not applicable.
Figures




References
-
- Statistisches Bundesamt, [Destatis]—Zentraler Auskunftsdienst, Wiesbaden. Krankenhausstatistik—Diagnosedaten der Patienten und Patientinnen in Krankenhäusern. https://www.gbe-bund.de. Accessed 30 Dec 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
