

Dysregulated hematopoiesis in bone marrow marks severe COVID-19
- PMID: 34349096
- PMCID: PMC8335717
- DOI: 10.1038/s41421-021-00296-9
Dysregulated hematopoiesis in bone marrow marks severe COVID-19
Abstract
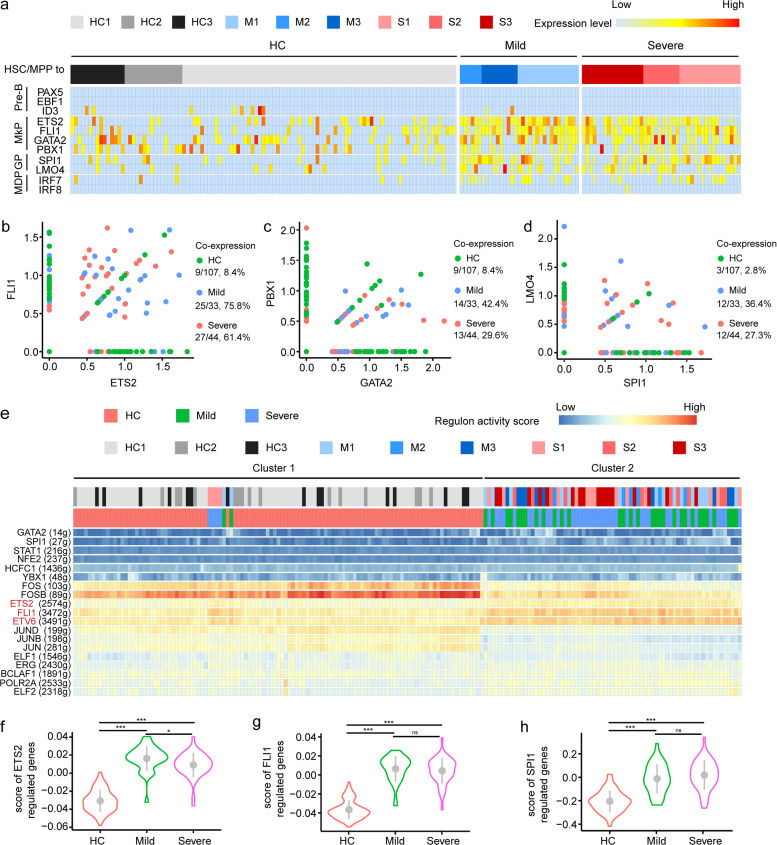
Severe coronavirus disease 2019 (COVID-19) is often indicated by lymphopenia and increased myelopoiesis; however, the underlying mechanism is still unclear, especially the alteration of hematopoiesis. It is important to explore to what extent and how hematopoietic stem cells contribute to the impairment of peripheral lymphoid and myeloid compartments in COVID-19 patients. In this study, we used single-cell RNA sequencing to assess bone marrow mononuclear cells from COVID-19 patients with peripheral blood mononuclear cells as control. The results showed that the hematopoietic stem cells in these patients were mainly in the G1 phase and prone to apoptosis, with immune activation and anti-viral responses. Importantly, a significant accumulation of immature myeloid progenitors and a dramatic reduction of lymphoid progenitors in severe cases were identified, along with the up-regulation of transcription factors (such as SPI1, LMO4, ETS2, FLI1, and GATA2) that are important for the hematopoietic stem cell or multipotent progenitor to differentiate into downstream progenitors. Our results indicate a dysregulated hematopoiesis in patients with severe COVID-19.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
Promotion of Expansion and Differentiation of Hematopoietic Stem Cells by Interleukin-27 into Myeloid Progenitors to Control Infection in Emergency Myelopoiesis.PLoS Pathog. 2016 Mar 18;12(3):e1005507. doi: 10.1371/journal.ppat.1005507. eCollection 2016 Mar. PLoS Pathog. 2016. PMID: 26991425 Free PMC article.
-
Sequencing of RNA in single cells reveals a distinct transcriptome signature of hematopoiesis in GATA2 deficiency.Blood Adv. 2020 Jun 23;4(12):2656-2670. doi: 10.1182/bloodadvances.2019001352. Blood Adv. 2020. PMID: 32556286 Free PMC article.
-
Low-level GATA2 overexpression promotes myeloid progenitor self-renewal and blocks lymphoid differentiation in mice.Exp Hematol. 2015 Jul;43(7):565-77.e1-10. doi: 10.1016/j.exphem.2015.04.002. Epub 2015 Apr 20. Exp Hematol. 2015. PMID: 25907033
-
[Quo vadis hematology?].Orv Hetil. 2016 Nov;157(46):1819-1829. doi: 10.1556/650.2016.30580. Orv Hetil. 2016. PMID: 27817226 Review. Hungarian.
-
Lymphoid and myeloid lineage commitment in multipotent hematopoietic progenitors.Immunol Rev. 2010 Nov;238(1):37-46. doi: 10.1111/j.1600-065X.2010.00963.x. Immunol Rev. 2010. PMID: 20969583 Free PMC article. Review.
Cited by
-
Nucleated red blood cells are a late biomarker in predicting intensive care unit mortality in patients with COVID-19 acute respiratory distress syndrome: an observational cohort study.Front Immunol. 2024 Jan 18;15:1313977. doi: 10.3389/fimmu.2024.1313977. eCollection 2024. Front Immunol. 2024. PMID: 38304431 Free PMC article.
-
Drug-Target Network Study Reveals the Core Target-Protein Interactions of Various COVID-19 Treatments.Genes (Basel). 2022 Jul 6;13(7):1210. doi: 10.3390/genes13071210. Genes (Basel). 2022. PMID: 35885993 Free PMC article.
-
The Functional Roles of MDSCs in Severe COVID-19 Pathogenesis.Viruses. 2023 Dec 23;16(1):27. doi: 10.3390/v16010027. Viruses. 2023. PMID: 38257728 Free PMC article. Review.
-
Hematopoietic responses to SARS-CoV-2 infection.Cell Mol Life Sci. 2022 Mar 13;79(3):187. doi: 10.1007/s00018-022-04220-6. Cell Mol Life Sci. 2022. PMID: 35284964 Free PMC article. Review.
-
Delineating COVID-19 immunological features using single-cell RNA sequencing.Innovation (Camb). 2022 Sep 13;3(5):100289. doi: 10.1016/j.xinn.2022.100289. Epub 2022 Jul 21. Innovation (Camb). 2022. PMID: 35879967 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
