

The role of Psl in the failure to eradicate Pseudomonas aeruginosa biofilms in children with cystic fibrosis
- PMID: 34349133
- PMCID: PMC8338932
- DOI: 10.1038/s41522-021-00234-3
The role of Psl in the failure to eradicate Pseudomonas aeruginosa biofilms in children with cystic fibrosis
Abstract
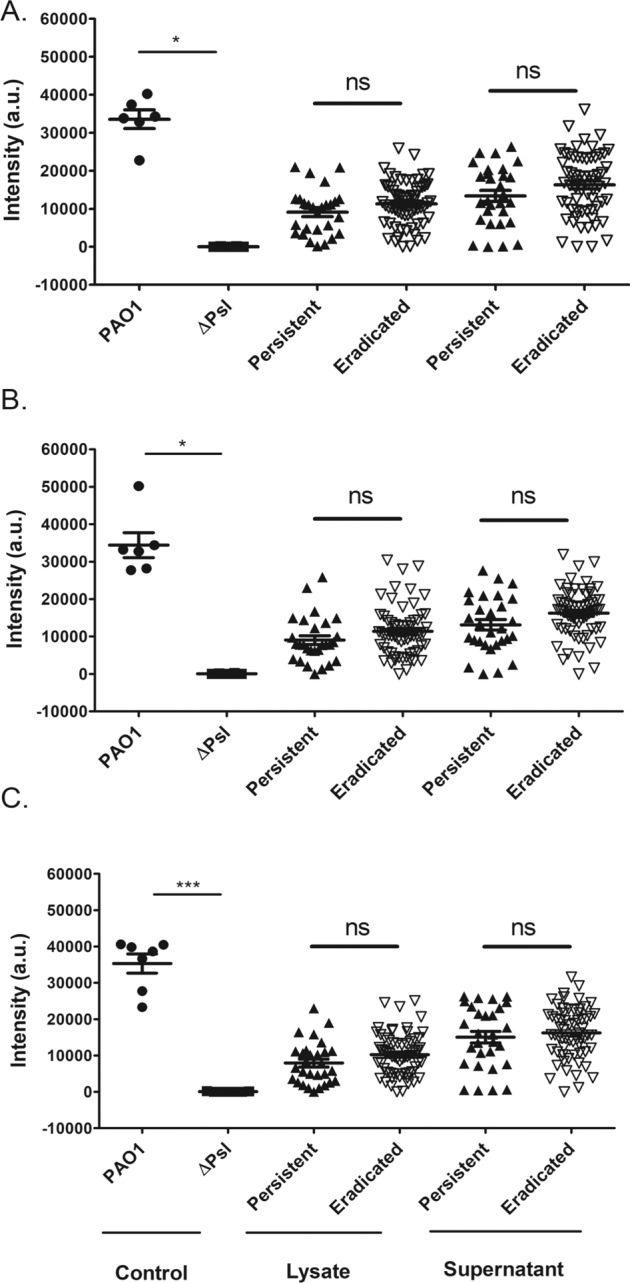
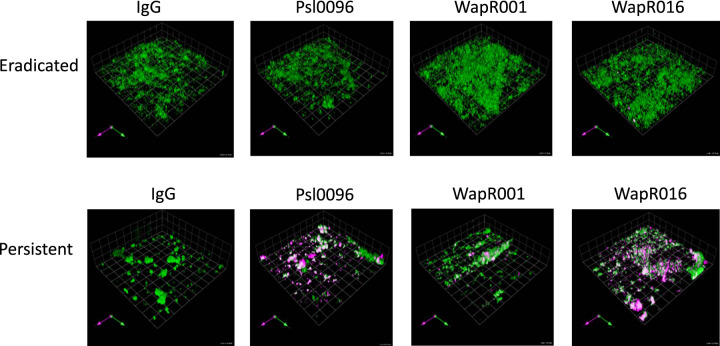
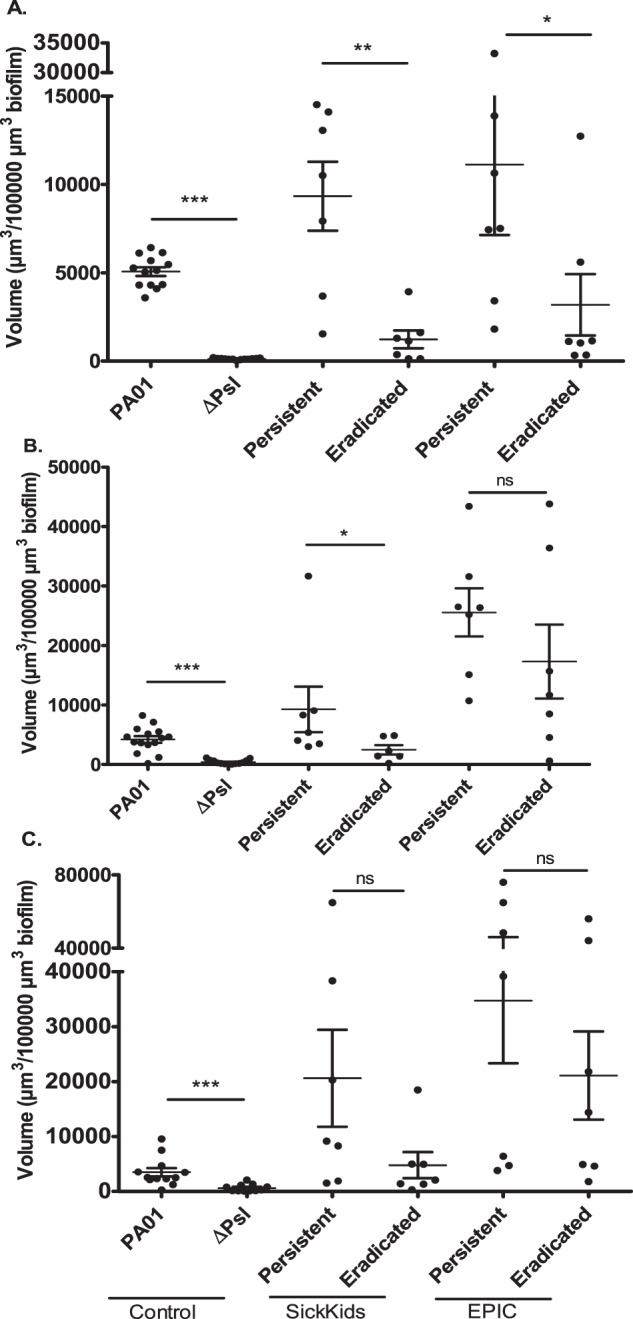
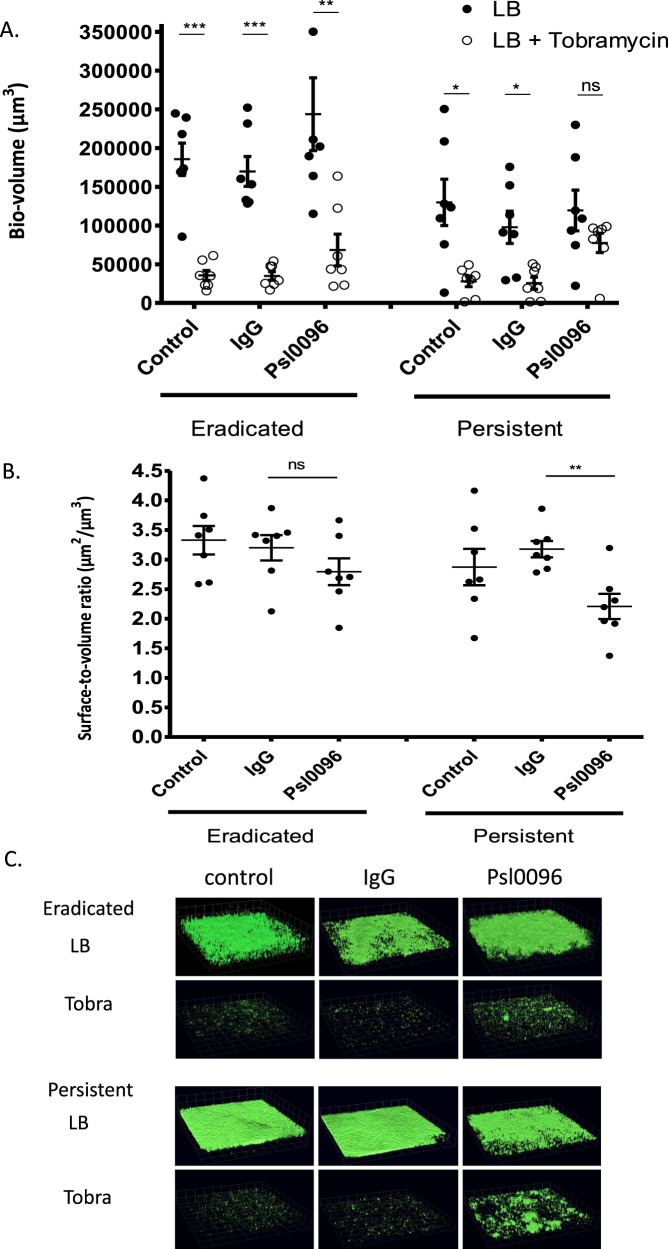
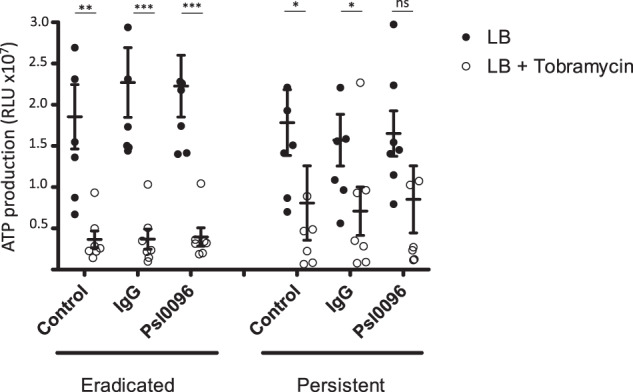
The exopolysaccharide Psl contributes to biofilm structure and antibiotic tolerance and may play a role in the failure to eradicate Pseudomonas aeruginosa from cystic fibrosis (CF) airways. The study objective was to determine whether there were any differences in Psl in P. aeruginosa isolates that were successfully eradicated compared to those that persisted, despite inhaled tobramycin treatment, in children with CF. Initial P. aeruginosa isolates were collected from children with CF undergoing eradication treatment, grown as biofilms and labeled with 3 anti-Psl monoclonal antibodies (Cam003/Psl0096, WapR001, WapR016) before confocal microscopy visualization. When grown as biofilms, P. aeruginosa isolates from children who failed antibiotic eradication therapy, had significantly increased Psl0096 binding compared to isolates from those who cleared P. aeruginosa. This was confirmed in P. aeruginosa isolates from the SickKids Eradication Cohort as well as the Early Pseudomonas Infection Control (EPIC) trial. Increased anti-Psl antibody binding was associated with bacterial aggregation and tobramycin tolerance. The biofilm matrix represents a potential therapeutic target to improve P. aeruginosa eradication treatment.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
