

Recent Updates in Neurosurgical Interventions for Spontaneous Intracerebral Hemorrhage: Minimally Invasive Surgery to Improve Surgical Performance
- PMID: 34349724
- PMCID: PMC8326326
- DOI: 10.3389/fneur.2021.703189
Recent Updates in Neurosurgical Interventions for Spontaneous Intracerebral Hemorrhage: Minimally Invasive Surgery to Improve Surgical Performance
Abstract
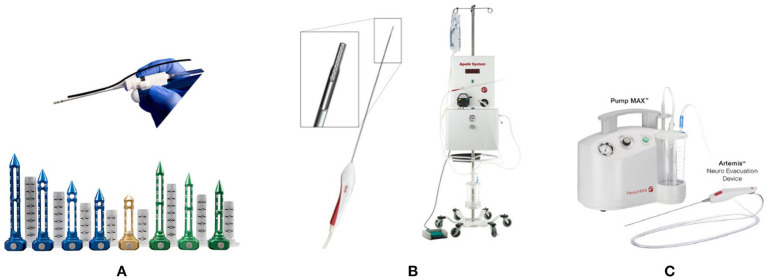
The efficacy and safety of surgical treatment for intracerebral hemorrhage (ICH) have long been subjects of investigation and debate. The recent results of the minimally invasive surgery plus alteplase for intracerebral hemorrhage evacuation (MISTIE) III trial demonstrated the safety of the procedure and a reduction in mortality compared to medical treatment. Although no improvement in functional outcomes was shown, the trial elucidated that benefits of intervention depend on surgical performance: a greater ICH reduction, defined as ≤ 15 mL end of treatment ICH volume or ≥70% volume reduction, correlated with significant functional improvement. Recent meta-analyses suggested the benefits of neurosurgical hematoma evacuation, especially when performed earlier and done using minimally invasive procedures. In MISTIE III, to confirm hemostasis and reduce the risk of rebleeding, the mean time from onset to surgery and treatment completion took 47 and 123 h, respectively. Theoretically, the earlier the hematoma is removed, the better the outcome. Therefore, a higher rate of hematoma reduction within an earlier time course may be beneficial. Neuroendoscopic surgery enables less invasive removal of ICH under direct visualization. Minimally invasive procedures have continued to evolve with the support of advanced guidance systems and devices in favor of better surgical performance. Ongoing randomized controlled trials utilizing emerging minimally invasive techniques, such as the Early Minimally Invasive Removal of Intra Cerebral Hemorrhage (ENRICH) trial, Minimally Invasive Endoscopic Surgical Treatment with Apollo/Artemis in Patients with Brain Hemorrhage (INVEST) trial, and the Dutch Intracerebral Hemorrhage Surgery Trial (DIST), may provide significant information on the optimal treatment for ICH.
Keywords: endoscopic surgery; intracerebral hemorrhage; minimally invasive surgery; stereotactic surgery; surgical performance; thrombolysis.
Copyright © 2021 Kobata and Ikeda.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Surgical Performance Determines Functional Outcome Benefit in the Minimally Invasive Surgery Plus Recombinant Tissue Plasminogen Activator for Intracerebral Hemorrhage Evacuation (MISTIE) Procedure.Neurosurgery. 2019 Jun 1;84(6):1157-1168. doi: 10.1093/neuros/nyz077. Neurosurgery. 2019. PMID: 30891610 Free PMC article. Clinical Trial.
-
Minimally Invasive Surgery for Intracerebral Hemorrhage.Curr Neurol Neurosci Rep. 2018 May 9;18(6):34. doi: 10.1007/s11910-018-0836-4. Curr Neurol Neurosci Rep. 2018. PMID: 29740726 Review.
-
What does the CT angiography "spot sign" of intracerebral hemorrhage mean in modern neurosurgical settings with minimally invasive endoscopic techniques?Neurosurg Rev. 2013 Jul;36(3):341-8. doi: 10.1007/s10143-012-0437-7. Epub 2012 Dec 16. Neurosurg Rev. 2013. PMID: 23242507 Review.
-
Surgical Performance in Minimally Invasive Surgery Plus Recombinant Tissue Plasminogen Activator for Intracerebral Hemorrhage Evacuation Phase III Clinical Trial.Neurosurgery. 2017 Nov 1;81(5):860-866. doi: 10.1093/neuros/nyx123. Neurosurgery. 2017. PMID: 28402516 Free PMC article. Clinical Trial.
-
Identifying Predictors of Initial Surgical Failure during Minimally Invasive Endoscopic Intracerebral Hemorrhage Evacuation.Biomedicines. 2024 Feb 23;12(3):508. doi: 10.3390/biomedicines12030508. Biomedicines. 2024. PMID: 38540121 Free PMC article.
Cited by
-
Outcome after Intracerebral Haemorrhage and Decompressive Craniectomy in Older Adults.Neurol Int. 2024 May 20;16(3):590-604. doi: 10.3390/neurolint16030044. Neurol Int. 2024. PMID: 38804483 Free PMC article.
-
Berberine mitigates intracerebral hemorrhage-induced neuroinflammation in a gut microbiota-dependent manner in mice.Aging (Albany NY). 2023 Apr 7;15(7):2705-2720. doi: 10.18632/aging.204642. Epub 2023 Apr 7. Aging (Albany NY). 2023. PMID: 37036515 Free PMC article.
-
Treatment outcomes between endoscopic surgery and conventional craniotomy for spontaneous supratentorial intracerebral hemorrhage: a randomized controlled trial.Neurosurg Rev. 2023 Jun 6;46(1):136. doi: 10.1007/s10143-023-02035-y. Neurosurg Rev. 2023. PMID: 37278839 Clinical Trial.
-
Neuroendoscopic Parafascicular Evacuation of Spontaneous Intracerebral Hemorrhage (NESICH Technique): A Multicenter Technical Experience with Preliminary Findings.Neurol Ther. 2024 Aug;13(4):1259-1271. doi: 10.1007/s40120-024-00642-5. Epub 2024 Jun 24. Neurol Ther. 2024. PMID: 38914793 Free PMC article.
-
Preoperative detailed evaluation intracranial artery stenosis using three-dimensional visualization analysis reduces the invasiveness of superficial temporal artery-middle cerebral artery bypass.Fujita Med J. 2023 Aug;9(3):206-210. doi: 10.20407/fmj.2022-022. Epub 2022 Dec 27. Fujita Med J. 2023. PMID: 37554939 Free PMC article.
References
-
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, et al. . Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet Glob Health. (2013) 1:e259–81. 10.1016/S2214-109X(13)70089-5 - DOI - PMC - PubMed
-
- Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, et al. . Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. (2005) 365:387–97. 10.1016/S0140-6736(05)17826-X - DOI - PubMed
-
- Mendelow AD, Gregson BA, Rowan EN, Murray GD, Gholkar A, Mitchell PM, et al. . Early surgery vs. initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): a randomised trial. Lancet. (2013) 382:397–408. 10.1016/S0140-6736(13)60986-1 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources