

Occurrence and timing of withdrawal of life-sustaining measures in traumatic brain injury patients: a CENTER-TBI study
- PMID: 34351445
- PMCID: PMC8486724
- DOI: 10.1007/s00134-021-06484-1
Occurrence and timing of withdrawal of life-sustaining measures in traumatic brain injury patients: a CENTER-TBI study
Abstract
Background: In patients with severe brain injury, withdrawal of life-sustaining measures (WLSM) is common in intensive care units (ICU). WLSM constitutes a dilemma: instituting WLSM too early could result in death despite the possibility of an acceptable functional outcome, whereas delaying WLSM could unnecessarily burden patients, families, clinicians, and hospital resources. We aimed to describe the occurrence and timing of WLSM, and factors associated with timing of WLSM in European ICUs in patients with traumatic brain injury (TBI).
Methods: The CENTER-TBI Study is a prospective multi-center cohort study. For the current study, patients with traumatic brain injury (TBI) admitted to the ICU and aged 16 or older were included. Occurrence and timing of WLSM were documented. For the analyses, we dichotomized timing of WLSM in early (< 72 h after injury) versus later (≥ 72 h after injury) based on recent guideline recommendations. We assessed factors associated with initiating WLSM early versus later, including geographic region, center, patient, injury, and treatment characteristics with univariable and multivariable (mixed effects) logistic regression.
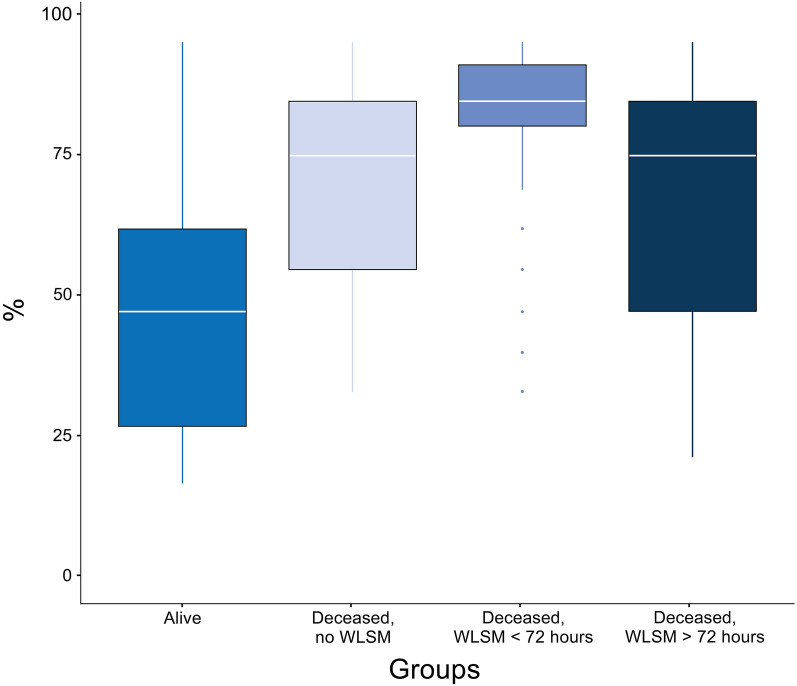
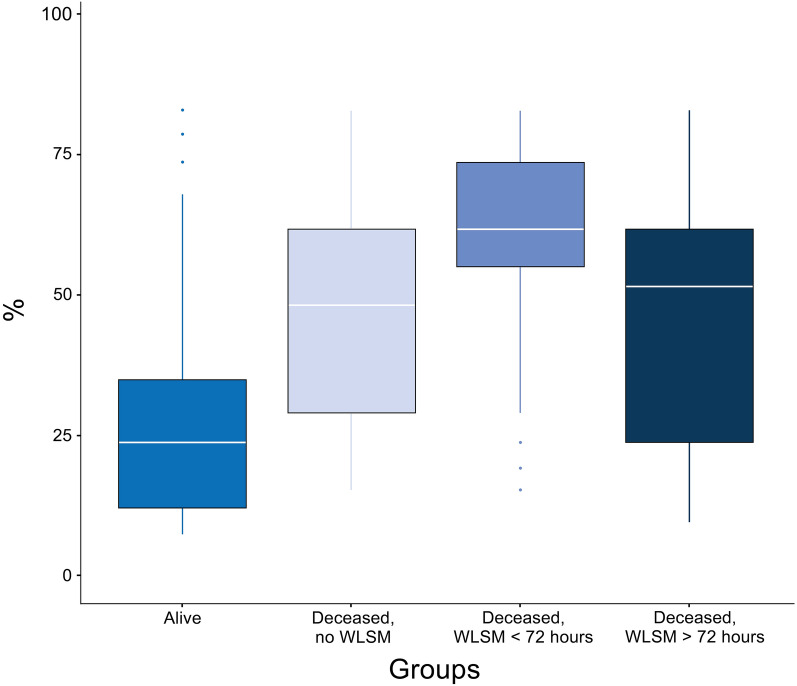
Results: A total of 2022 patients aged 16 or older were admitted to the ICU. ICU mortality was 13% (n = 267). Of these, 229 (86%) patients died after WLSM, and were included in the analyses. The occurrence of WLSM varied between regions ranging from 0% in Eastern Europe to 96% in Northern Europe. In 51% of the patients, WLSM was early. Patients in the early WLSM group had a lower maximum therapy intensity level (TIL) score than patients in the later WLSM group (median of 5 versus 10) The strongest independent variables associated with early WLSM were one unreactive pupil (odds ratio (OR) 4.0, 95% confidence interval (CI) 1.3-12.4) or two unreactive pupils (OR 5.8, CI 2.6-13.1) compared to two reactive pupils, and an Injury Severity Score (ISS) if over 41 (OR per point above 41 = 1.1, CI 1.0-1.1). Timing of WLSM was not significantly associated with region or center.
Conclusion: WLSM occurs early in half of the patients, mostly in patients with severe TBI affecting brainstem reflexes who were severely injured. We found no regional or center influences in timing of WLSM. Whether WLSM is always appropriate or may contribute to a self-fulfilling prophecy requires further research and argues for reluctance to institute WLSM early in case of any doubt on prognosis.
Keywords: Critical care; Intensive care unit; Traumatic brain injury; WLSM.
© 2021. The Author(s).
Conflict of interest statement
GC is Editor-in-Chief of Intensive Care Medicine. GC reports grants, personal fees as Speakers’ Bureau Member and Advisory Board Member from Integra and Neuroptics; personal fees from Nestle and UCB Pharma, all outside of the submitted work. DKM reports grants from the European Union and UK National Institute for Health Research, during the conduct of the study; grants, personal fees, and non-financial support from GlaxoSmithKline; personal fees from Neurotrauma Sciences, Lantmaanen AB, Pressura, and Pfizer, outside of the submitted work. The other authors declare that they have no competing interests.
Figures
References
-
- van Veen E, van der Jagt M, Citerio G, Stocchetti N, Epker JL, Gommers D, Burdorf L, Menon DK, Maas AIR, Lingsma HF, Kompanje EJO, investigators C-T,participants End-of-life practices in traumatic brain injury patients: Report of a questionnaire from the CENTER-TBI study. J Crit Care. 2020;58:78–88. doi: 10.1016/j.jcrc.2020.04.001. - DOI - PubMed
