

Prognostic Model for De Novo and Recurrent Metastatic Breast Cancer
- PMID: 34351787
- PMCID: PMC8807018
- DOI: 10.1200/CCI.21.00020
Prognostic Model for De Novo and Recurrent Metastatic Breast Cancer
Abstract
Purpose: Metastatic breast cancer (MBC) has a heterogeneous clinical course. We sought to develop a prognostic model for overall survival (OS) that incorporated contemporary tumor and clinical factors for estimating individual prognosis.
Methods: We identified patients with MBC from our institution diagnosed between 1998 and 2017. We developed OS prognostic models by Cox regression using demographic, tumor, and treatment variables. We assessed model predictive accuracy and estimated annual OS probabilities. We evaluated model discrimination and prediction calibration using an external validation data set from the National Comprehensive Cancer Network.
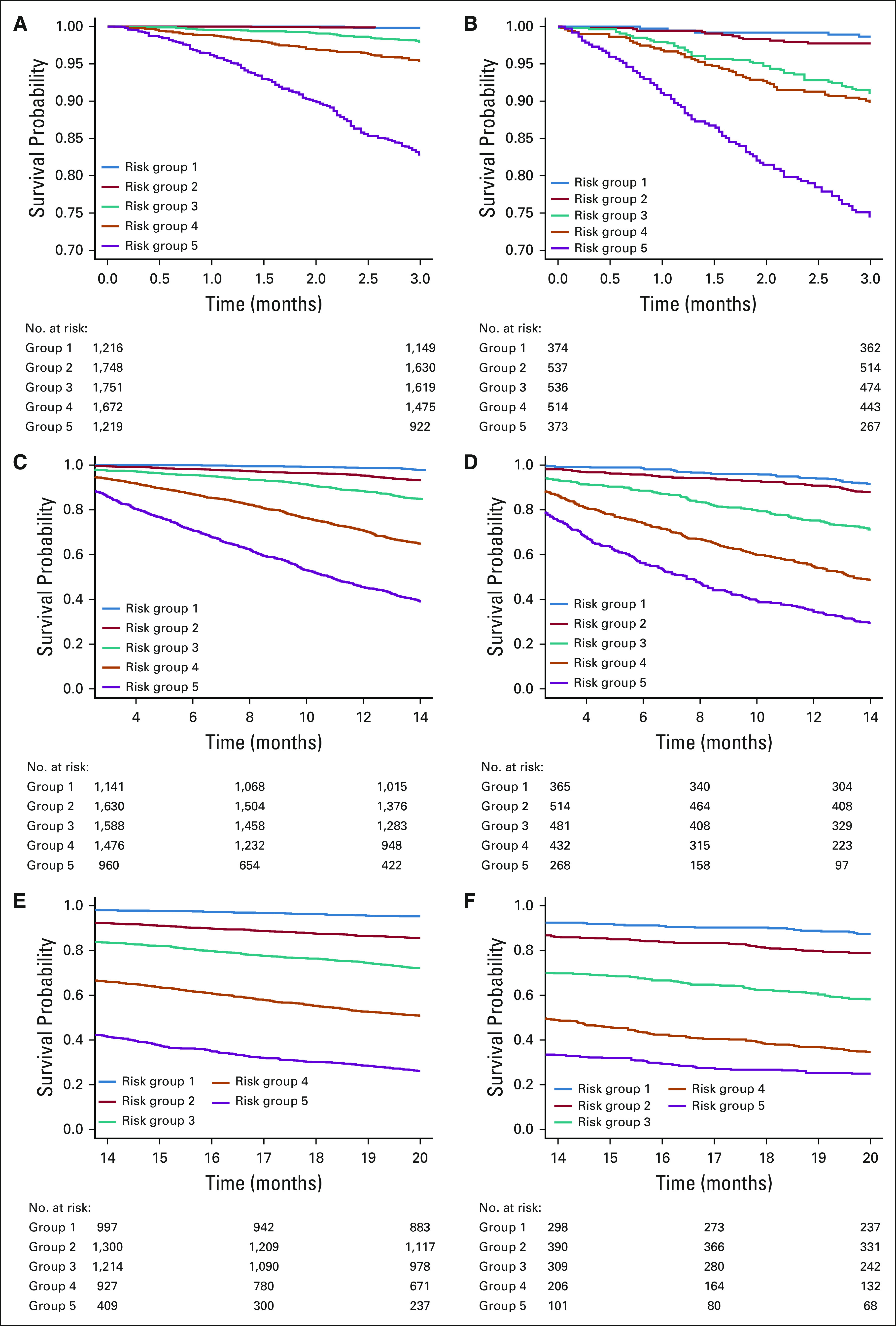
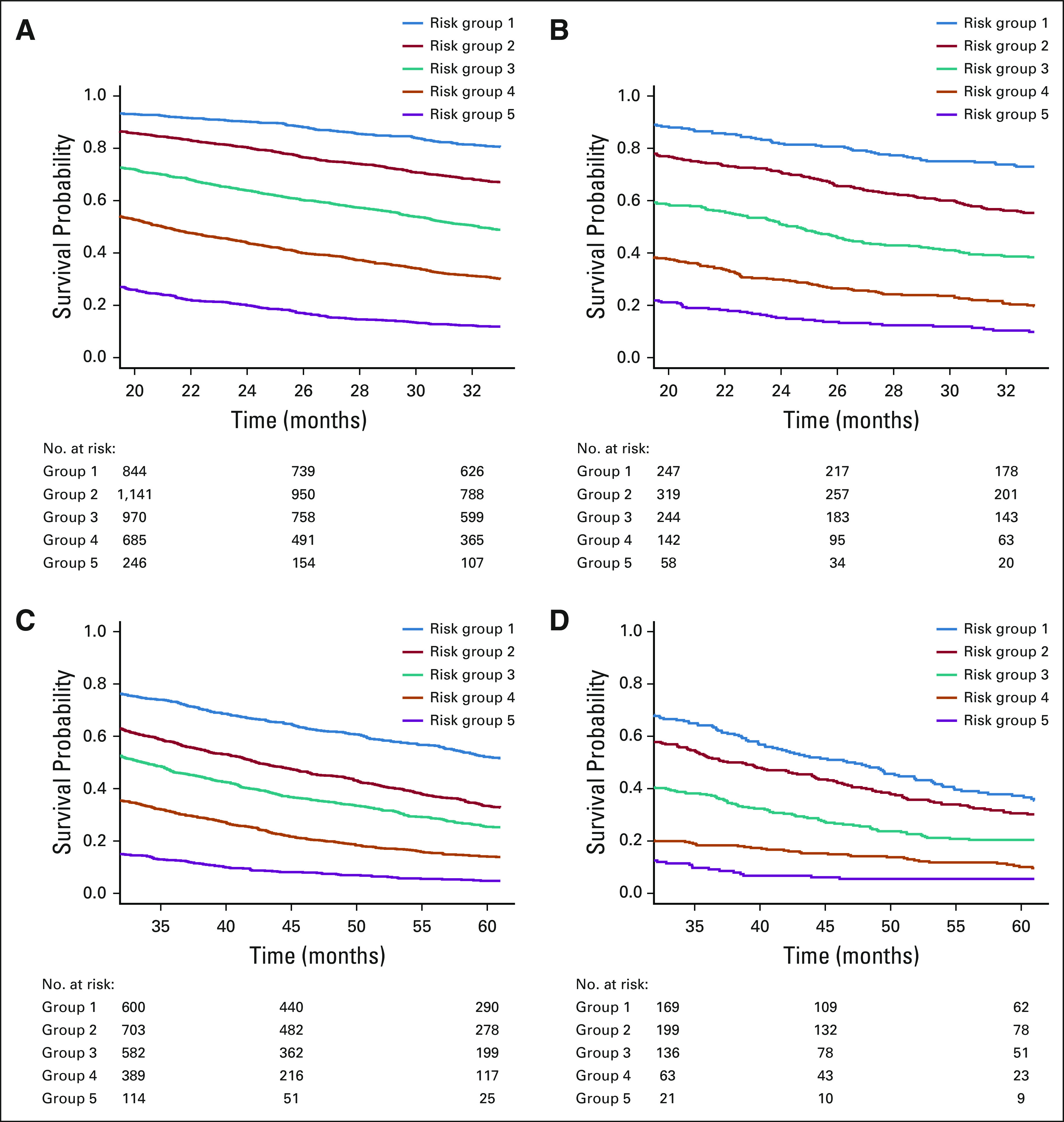
Results: We identified 10,655 patients. A model using age at diagnosis, race or ethnicity, hormone receptor and human epidermal growth factor receptor 2 subtype, de novo versus recurrent MBC categorized by metastasis-free interval, Karnofsky performance status, organ involvement, frontline biotherapy, frontline hormone therapy, and the interaction between variables significantly improved predictive accuracy (C-index, 0.731; 95% CI, 0.724 to 0.739) compared with a model with only hormone receptor and human epidermal growth factor receptor 2 status (C-index, 0.617; 95% CI, 0.609 to 0.626). The extended Cox regression model consisting of six independent models, for < 3, 3-14, 14-20, 20-33, 33-61, and ≥ 61 months, estimated up to 5 years of annual OS probabilities. The selected multifactor model had good discriminative ability but suboptimal calibration in the group of 2,334 National Comprehensive Cancer Network patients. A recalibration model that replaced the baseline survival function with the average of those from the training and validation data improved predictions across both data sets.
Conclusion: We have generated and validated a robust prognostic OS model for MBC. This model can be used in clinical decision making and stratification in clinical trials.
Conflict of interest statement
Figures
Comment in
-
Systematic Bias in Medical Algorithms: To Include or Not Include Discriminatory Demographic Information?JCO Clin Cancer Inform. 2022 Feb;6:e2100146. doi: 10.1200/CCI.21.00146. JCO Clin Cancer Inform. 2022. PMID: 35175859 No abstract available.
-
Reply to A. Pfob and C. Sidey-Gibbons.JCO Clin Cancer Inform. 2022 Feb;6:e2100171. doi: 10.1200/CCI.21.00171. JCO Clin Cancer Inform. 2022. PMID: 35175860 No abstract available.
References
-
- Ernst MF, van de Poll-Franse LV, Roukema JA, et al. Trends in the prognosis of patients with primary metastatic breast cancer diagnosed between 1975 and 2002 Breast 16344–3512007 - PubMed
-
- Bertaut A, Mounier M, Desmoulins I, et al. Stage IV breast cancer: A population‐based study about prognostic factors according to HER 2 and HR status Eur J Cancer Care 24920–9282015 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
