

Prevalence of fibrodysplasia ossificans progressiva (FOP) in the United States: estimate from three treatment centers and a patient organization
- PMID: 34353327
- PMCID: PMC8340531
- DOI: 10.1186/s13023-021-01983-2
Prevalence of fibrodysplasia ossificans progressiva (FOP) in the United States: estimate from three treatment centers and a patient organization
Abstract
Background: Fibrodysplasia ossificans progressiva (FOP), an ultra-rare, progressive, and permanently disabling disorder of extraskeletal ossification, is characterized by episodic and painful flare-ups and irreversible heterotopic ossification in muscles, tendons, and ligaments. Prevalence estimates have been hindered by the rarity of FOP and the heterogeneity of disease presentation. This study aimed to provide a baseline prevalence of FOP in the United States, based on contact with one of 3 leading treatment centers for FOP (University of Pennsylvania, Mayo Clinic, or University of California San Francisco), the International Fibrodysplasia Ossificans Progressiva Association (IFOPA) membership list, or the IFOPA FOP Registry through July 22, 2020.
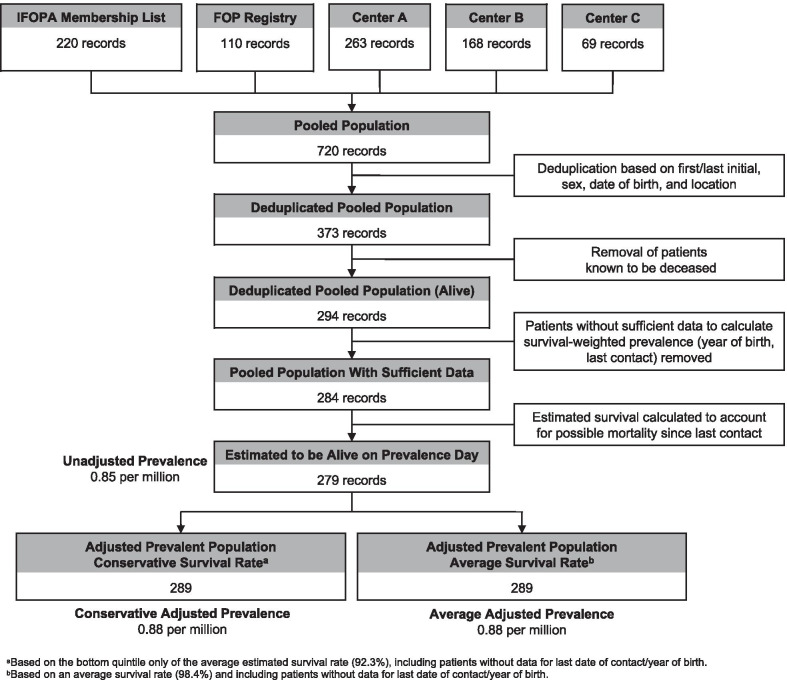
Results: Patient records were reviewed, collected, and deduplicated using first and last name initials, sex, state, and year of birth. A Kaplan-Meier survival curve was applied to each individual patient to estimate the probability that he or she was still alive, and a probability-weighted net prevalence estimate was calculated. After deduplication, 373 unique patients were identified in the United States, 294 of whom who were not listed as deceased in any list. The average time since last contact for 284 patients was 1.5 years. Based on the application of the survival probability, it is estimated that 279 of these patients were alive on the prevalence date (22 July 2020). An adjusted prevalence of 0.88 per million US residents was calculated using either an average survival rate estimate of 98.4% or a conservative survival rate estimate of 92.3% (based on the Kaplan-Meier survival curve from a previous study) and the US Census 2020 estimate of 329,992,681 on prevalence day.
Conclusions: This study suggests that the prevalence of FOP is higher than the often-cited value of 0.5 per million. Even so, because inclusion in this study was contingent upon treatment by the authors, IFOPA membership with confirmed clinical diagnosis, and the FOP Registry, the prevalence of FOP in the US may be higher than that identified here. Thus, it is imperative that efforts be made to identify and provide expert care for patients with this ultra-rare, significantly debilitating disease.
Keywords: ACVR1; Epidemiology; FOP; Fibrodysplasia ossificans progressiva; Heterotopic ossification; Prevalence; Rare disease.
© 2021. The Author(s).
Conflict of interest statement
None of the authors have competing interests to report. Robert J. Pignolo: Research investigator: Clementia/Ipsen, Regeneron; Advisory board: President of the International Clinical Council on FOP. Edward C. Hsiao: Research Investigator, Clementia/Ipsen; Prior research support from Regeneron. And Neurocrine Biosciences. Volunteer service on the IFOPA Medical Registry Advisory Board, the Fibrous Dysplasia Foundation Medical Advisory Board, and the International Clinical Council (ICC) of FOP. Genevieve Baujat: Research Investigator Ipsen, Regeneron, member of the International Clinical Council (ICC) of FOP, European Council for FOP and FOP France Medical Advisory Board. David Lapidus: David Ladipus was paid as a consultant by IFOPA for his work in compiling data. Prior consultant for Clementia (role ended in September, 2019). Adam Sherman: None. Frederick S. Kaplan: Research investigator: Ipsen & Regeneron; IFOPA Medical Advisory Board; Founder and Immediate Past-President of the International Clinical Council (ICC) on FOP; Chair of the Publications Committee of the ICC.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
