

Dexamethasone and tocilizumab treatment considerably reduces the value of C-reactive protein and procalcitonin to detect secondary bacterial infections in COVID-19 patients
- PMID: 34353339
- PMCID: PMC8340482
- DOI: 10.1186/s13054-021-03717-z
Dexamethasone and tocilizumab treatment considerably reduces the value of C-reactive protein and procalcitonin to detect secondary bacterial infections in COVID-19 patients
Abstract
Background: Procalcitonin (PCT) and C-reactive protein (CRP) were previously shown to have value for the detection of secondary infections in critically ill COVID-19 patients. However, since the introduction of immunomodulatory therapy, the value of these biomarkers is unclear. We investigated PCT and CRP kinetics in critically ill COVID-19 patients treated with dexamethasone with or without tocilizumab, and assessed the value of these biomarkers to detect secondary bacterial infections.
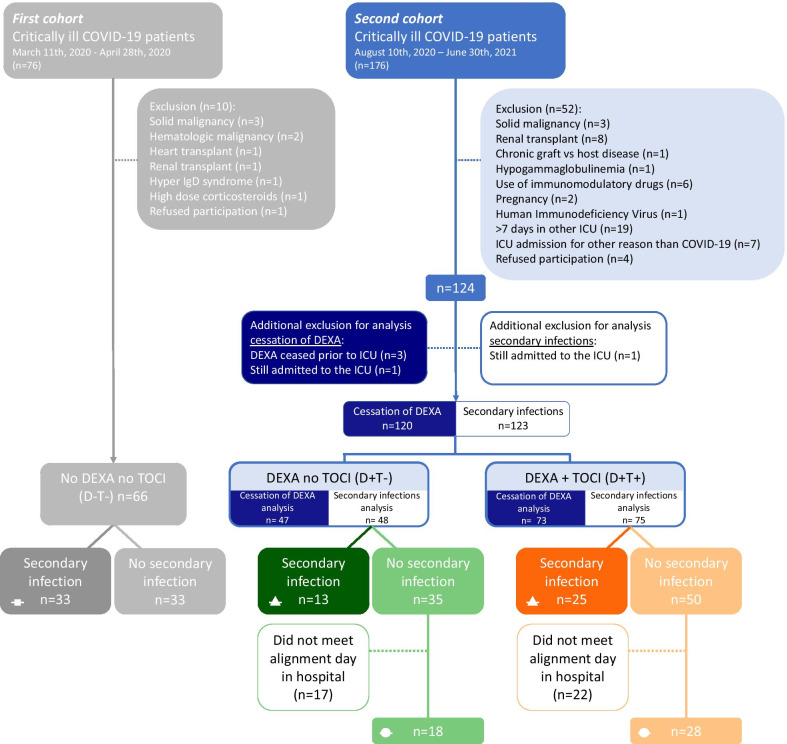
Methods: In this prospective study, 190 critically ill COVID-19 patients were divided into three treatment groups: no dexamethasone, no tocilizumab (D-T-), dexamethasone, no tocilizumab (D+T-), and dexamethasone and tocilizumab (D+T+). Serial data of PCT and CRP were aligned on the last day of dexamethasone treatment, and kinetics of these biomarkers were analyzed between 6 days prior to cessation of dexamethasone and 10 days afterwards. Furthermore, the D+T- and D+T+ groups were subdivided into secondary infection and no-secondary infection groups to analyze differences in PCT and CRP kinetics and calculate detection accuracy of these biomarkers for the occurrence of a secondary infection.
Results: Following cessation of dexamethasone, there was a rebound in PCT and CRP levels, most pronounced in the D+T- group. Upon occurrence of a secondary infection, no significant increase in PCT and CRP levels was observed in the D+T- group (p = 0.052 and p = 0.08, respectively). Although PCT levels increased significantly in patients of the D+T+ group who developed a secondary infection (p = 0.0003), this rise was only apparent from day 2 post-infection onwards. CRP levels remained suppressed in the D+T+ group. Receiver operating curve analysis of PCT and CRP levels yielded area under the curves of 0.52 and 0.55, respectively, which are both markedly lower than those found in the group of COVID-19 patients not treated with immunomodulatory drugs (0.80 and 0.76, respectively, with p values for differences between groups of 0.001 and 0.02, respectively).
Conclusions: Cessation of dexamethasone in critically ill COVID-19 patients results in a rebound increase in PCT and CRP levels unrelated to the occurrence of secondary bacterial infections. Furthermore, immunomodulatory treatment with dexamethasone and tocilizumab considerably reduces the value of PCT and CRP for detection of secondary infections in COVID-19 patients.
Keywords: COVID-19; Dexamethasone; Prediction; Procalcitonin; Tocilizumab; c-reactive protein.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests related to this study.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
