

Rapid Exclusion of COVID Infection With the Artificial Intelligence Electrocardiogram
- PMID: 34353468
- PMCID: PMC8327278
- DOI: 10.1016/j.mayocp.2021.05.027
Rapid Exclusion of COVID Infection With the Artificial Intelligence Electrocardiogram
Abstract
Objective: To rapidly exclude severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection using artificial intelligence applied to the electrocardiogram (ECG).
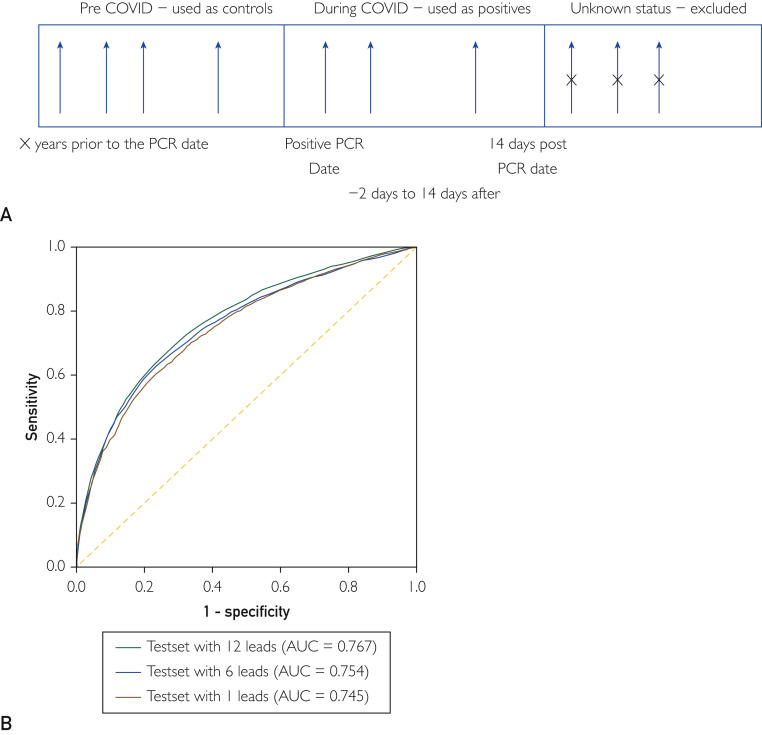
Methods: A global, volunteer consortium from 4 continents identified patients with ECGs obtained around the time of polymerase chain reaction-confirmed COVID-19 diagnosis and age- and sex-matched controls from the same sites. Clinical characteristics, polymerase chain reaction results, and raw electrocardiographic data were collected. A convolutional neural network was trained using 26,153 ECGs (33.2% COVID positive), validated with 3826 ECGs (33.3% positive), and tested on 7870 ECGs not included in other sets (32.7% positive). Performance under different prevalence values was tested by adding control ECGs from a single high-volume site.
Results: The area under the curve for detection of acute COVID-19 infection in the test group was 0.767 (95% CI, 0.756 to 0.778; sensitivity, 98%; specificity, 10%; positive predictive value, 37%; negative predictive value, 91%). To more accurately reflect a real-world population, 50,905 normal controls were added to adjust the COVID prevalence to approximately 5% (2657/58,555), resulting in an area under the curve of 0.780 (95% CI, 0.771 to 0.790) with a specificity of 12.1% and a negative predictive value of 99.2%.
Conclusion: Infection with SARS-CoV-2 results in electrocardiographic changes that permit the artificial intelligence-enhanced ECG to be used as a rapid screening test with a high negative predictive value (99.2%). This may permit the development of electrocardiography-based tools to rapidly screen individuals for pandemic control.
Copyright © 2021. Published by Elsevier Inc.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
