

Imaging of Neuromodulation and Surgical Interventions for Epilepsy
- PMID: 34353787
- PMCID: PMC8562735
- DOI: 10.3174/ajnr.A7222
Imaging of Neuromodulation and Surgical Interventions for Epilepsy
Abstract
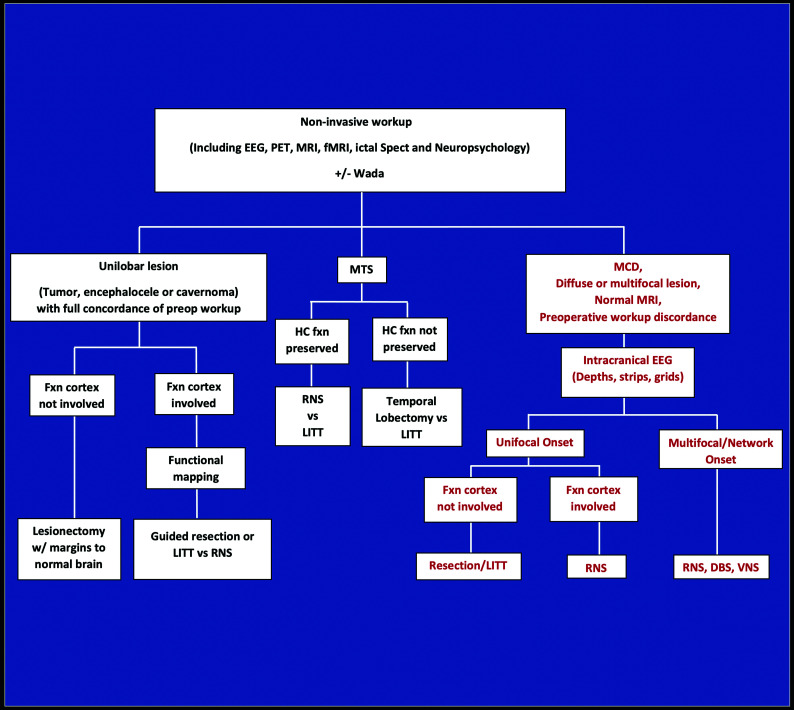
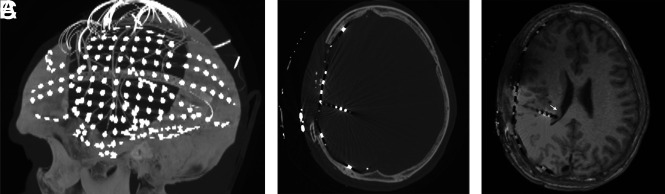
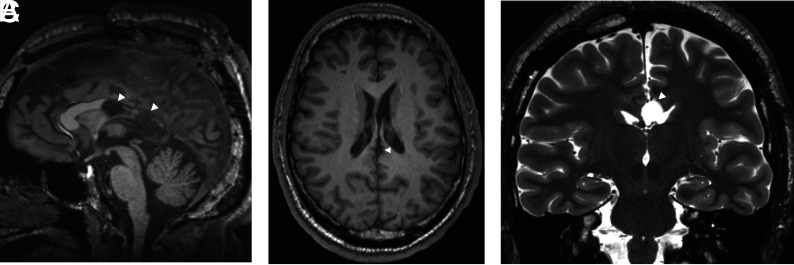
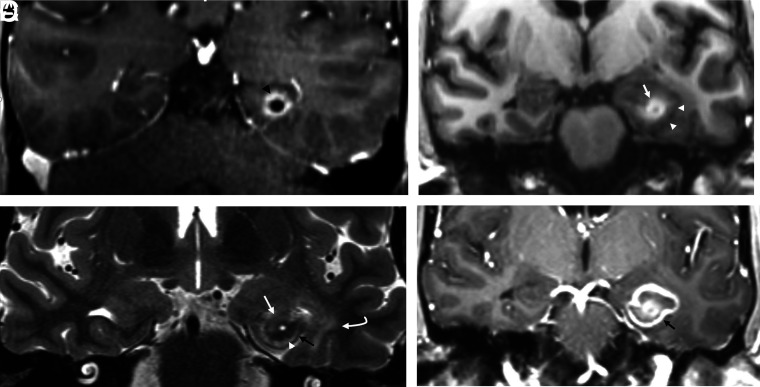
About one-third of epilepsy cases are refractory to medical therapy. During the past decades, the availability of surgical epilepsy interventions has substantially increased as therapeutic options for this group of patients. A wide range of surgical interventions and electrophysiologic neuromodulation techniques are available, including lesional resection, lobar resection, thermoablation, disconnection, multiple subpial transections, vagus nerve stimulation, responsive neurostimulation, and deep brain stimulation. The indications and imaging features of potential complications of the newer surgical interventions may not be widely appreciated, particularly if practitioners are not associated with comprehensive epilepsy centers. In this article, we review a wide range of invasive epilepsy treatment modalities with a particular focus on their postoperative imaging findings and complications. A state-of-the-art treatment algorithm provides context for imaging findings by helping the reader understand how a particular invasive treatment decision is made.
© 2021 by American Journal of Neuroradiology.
Figures


References
-
- Zentner J. Surgical Treatment of Epilepsies. In: Advances in Epilepsy Surgery and Radiosurgery. Springer, Vienna; 2002:27–35
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous