

A Wirelessly Controlled Smart Bandage with 3D-Printed Miniaturized Needle Arrays
- PMID: 34354556
- PMCID: PMC8336080
- DOI: 10.1002/adfm.201905544
A Wirelessly Controlled Smart Bandage with 3D-Printed Miniaturized Needle Arrays
Abstract
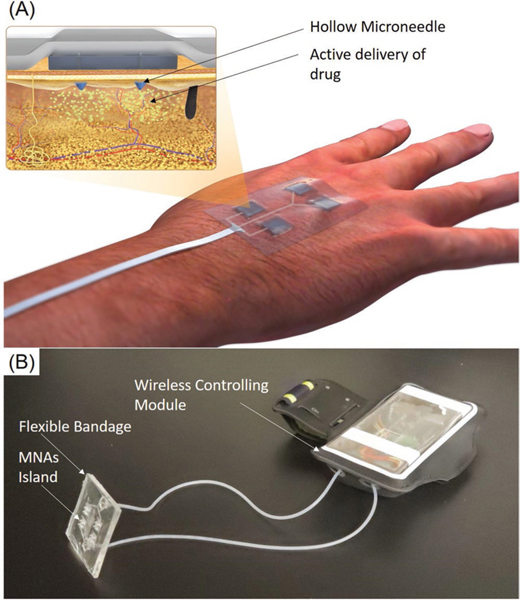
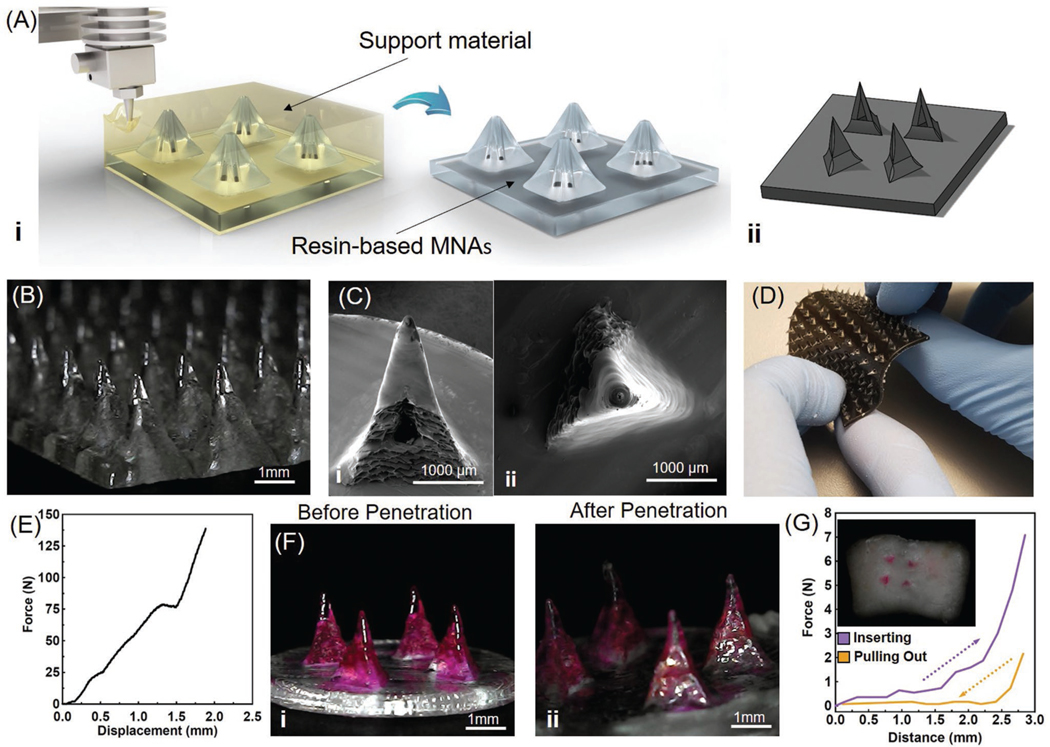
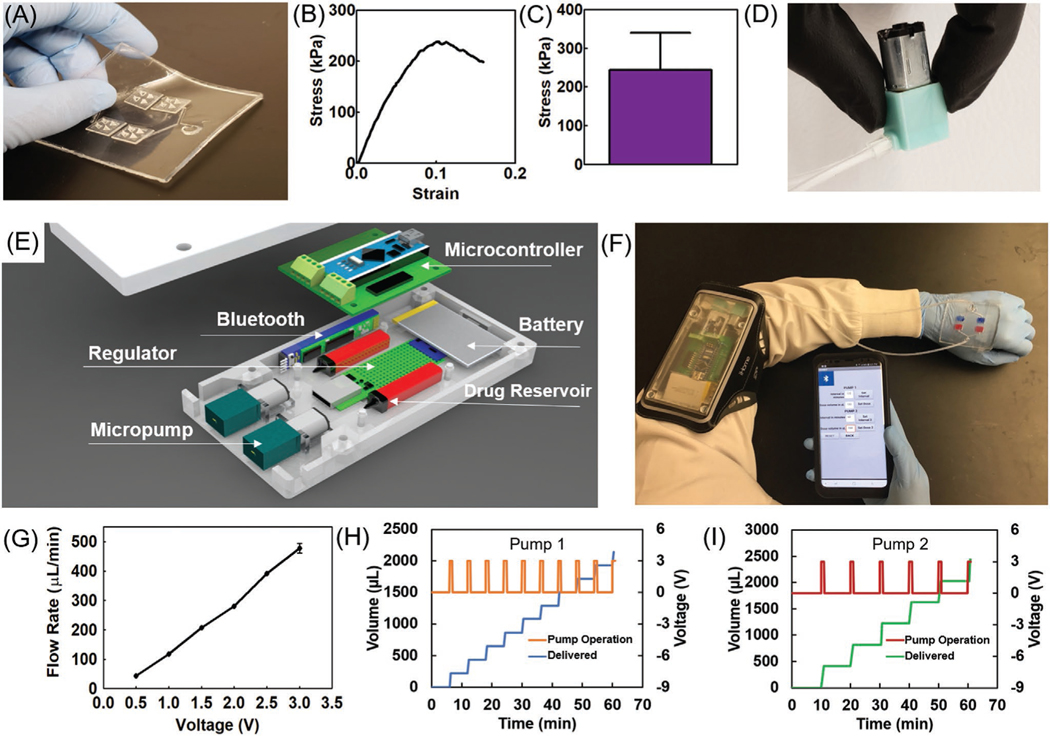
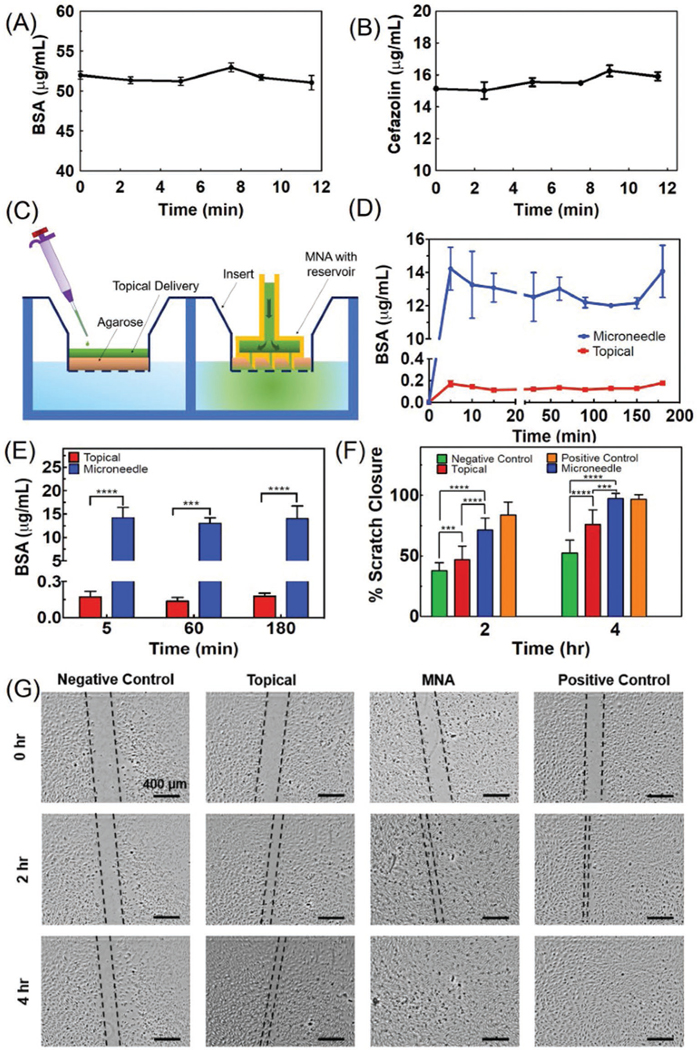
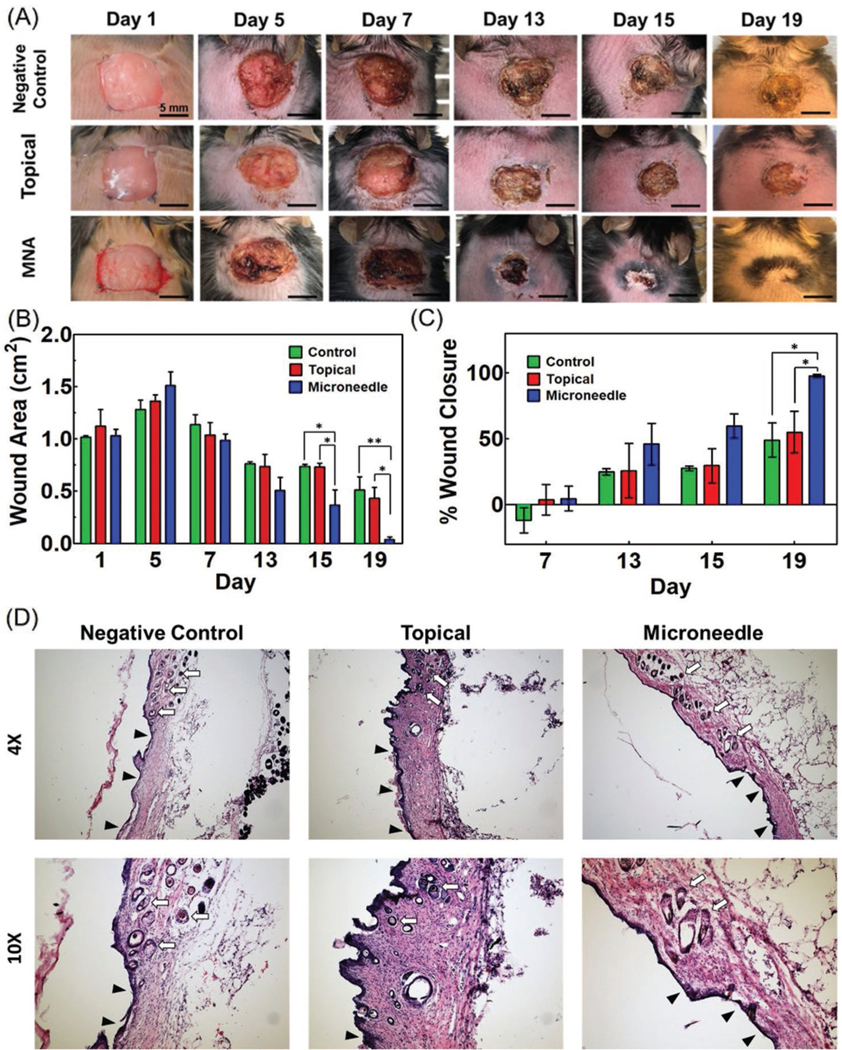
Chronic wounds are one of the most devastating complications of diabetes and are the leading cause of nontraumatic limb amputation. Despite the progress in identifying factors and promising in vitro results for the treatment of chronic wounds, their clinical translation is limited. Given the range of disruptive processes necessary for wound healing, different pharmacological agents are needed at different stages of tissue regeneration. This requires the development of wearable devices that can deliver agents to critical layers of the wound bed in a minimally invasive fashion. Here, for the first time, a programmable platform is engineered that is capable of actively delivering a variety of drugs with independent temporal profiles through miniaturized needles into deeper layers of the wound bed. The delivery of vascular endothelial growth factor (VEGF) through the miniaturized needle arrays demonstrates that, in addition to the selection of suitable therapeutics, the delivery method and their spatial distribution within the wound bed is equally important. Administration of VEGF to chronic dermal wounds of diabetic mice using the programmable platform shows a significant increase in wound closure, re-epithelialization, angiogenesis, and hair growth when compared to standard topical delivery of therapeutics.
Keywords: 3D-printed needles; active drug delivery; chronic wounds; smart bandages.
Conflict of interest statement
Conflict of Interest The authors declare no conflict of interest.
Figures
References
-
- Guo S, DiPietro LA, J. Dent. Res 2010, 89, 219; - PMC - PubMed
- Saghazadeh S, Rinoldi C, Schot M, Kashaf SS, Sharifi F, Jalilian E, Nuutila K, Giatsidis G, Mostafalu P, Derakhshandeh H, Yue K, Swieszkowski W, Memic A, Tamayol A, Khademhosseini A, Adv. Drug Delivery Rev 2018, 127, 138; - PMC - PubMed
- Guo J, Dardik A, Fang K, Huang R, Gu Y, Stem Cell Res. Ther 2017, 8, 228. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources