

Biologic Tuberoplasty With an Acellular Dermal Allograft for Massive Rotator Cuff Tears
- PMID: 34354916
- PMCID: PMC8322474
- DOI: 10.1016/j.eats.2021.03.016
Biologic Tuberoplasty With an Acellular Dermal Allograft for Massive Rotator Cuff Tears
Abstract
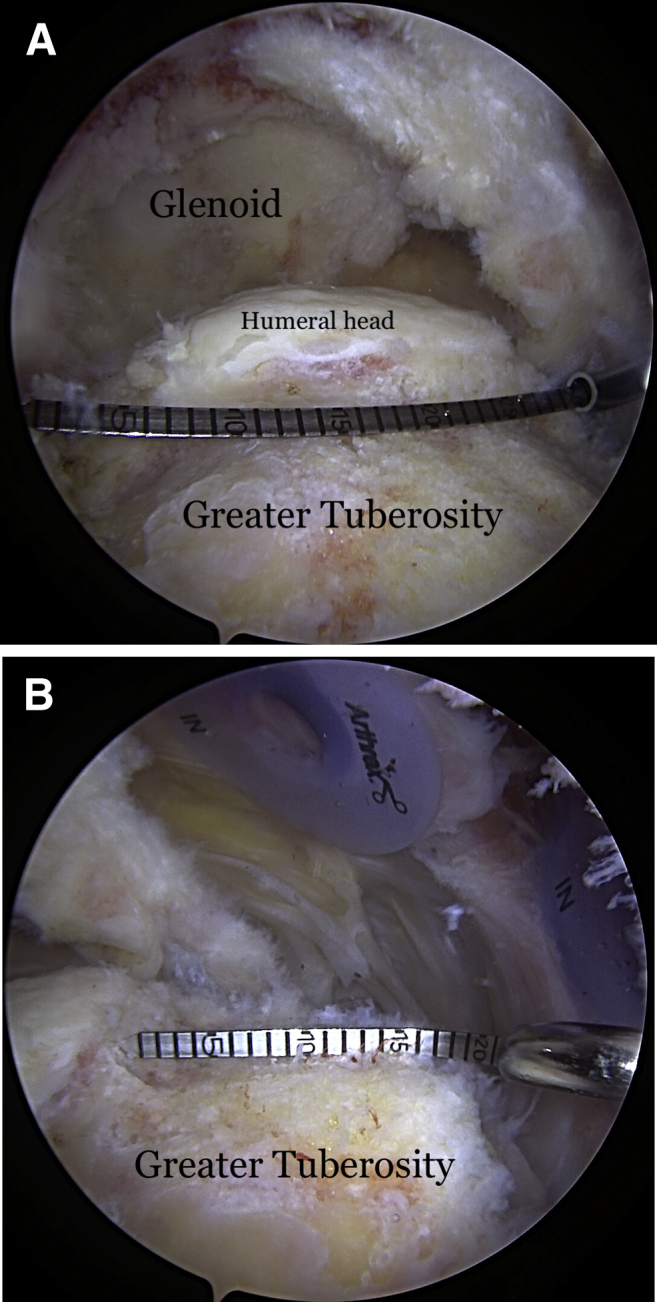
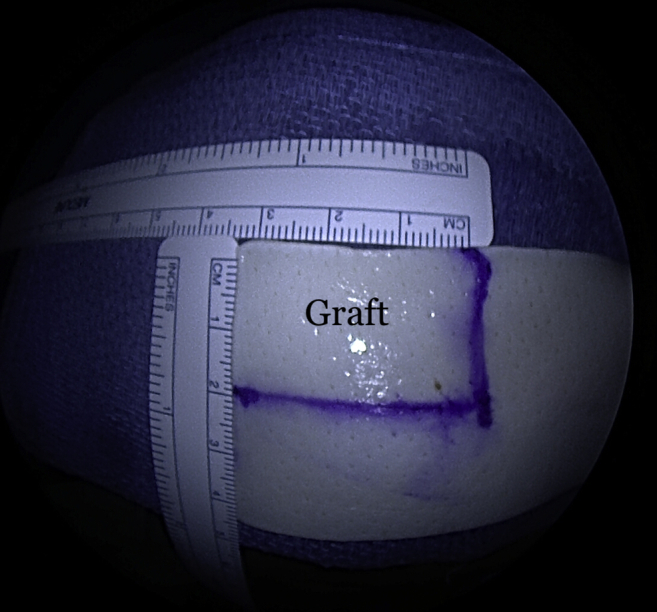
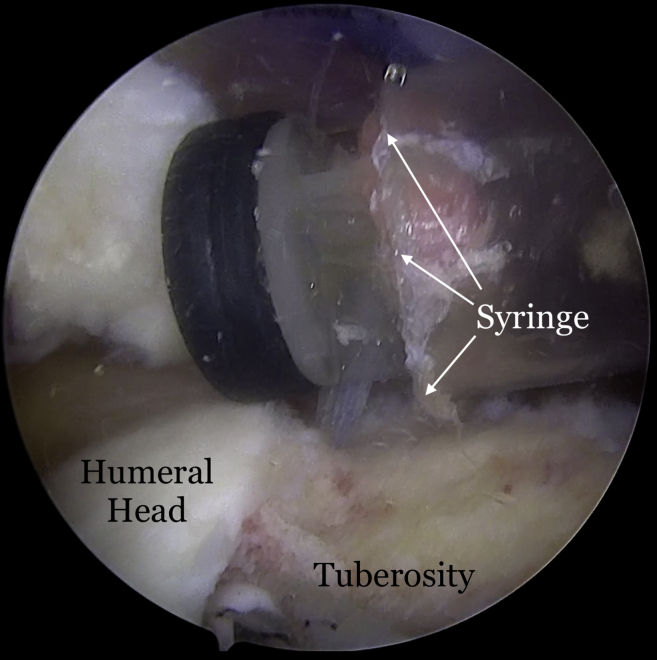
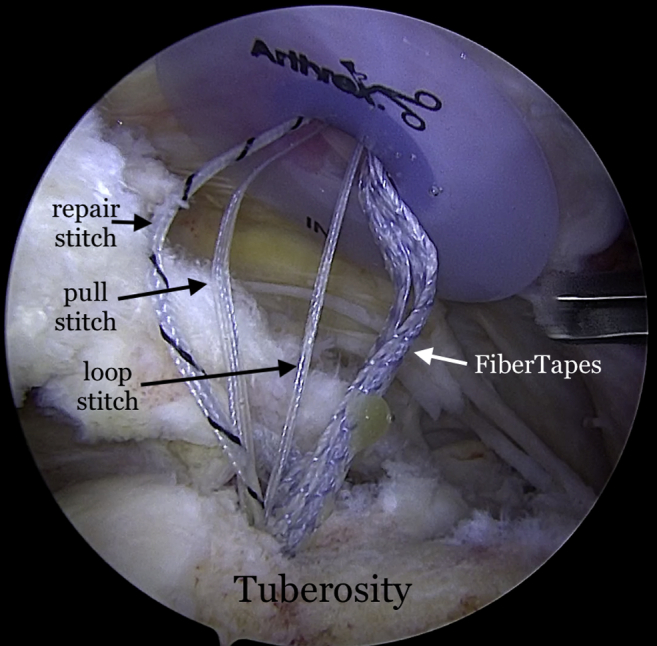
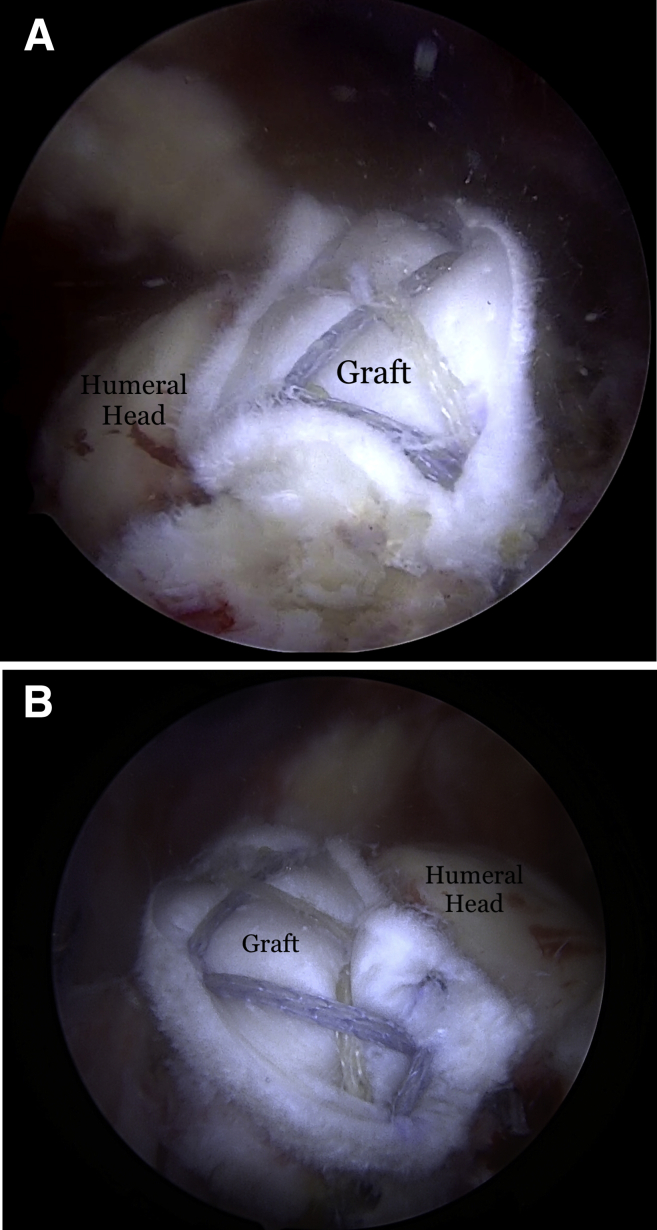
We present the technique of biologic tuberoplasty, where an acellular dermal allograft is used to cover the tuberosity in patients with massive irreparable cuff tears to prevent bone-to-bone contact between the tuberosity and acromion when active elevation is attempted. This technique can be performed in patients with massive rotator cuff tears who are low-demand and have significant medical comorbidities, poor bone quality, or who are not candidates for a reverse shoulder arthroplasty or who cannot tolerate a lengthy rehabilitation protocol. It is less time-consuming than a superior capsule reconstruction and more bone-sparing than traditional tuberoplasty. Patients with massive rotator cuff tears involving the supraspinatus and a portion of the infraspinatus lose their force couple, leading to superior humeral head migration with abutment of the tuberosity against the acromion upon deltoid activation. The center of rotation moves superiorly with deltoid contraction, developing an acromiohumeral articulation. This results in bone-to-bone contact between the acromion and humerus, leading to pain and acetabularization of the acromion over time. Coverage of the tuberosity with the acellular dermal allograft acts as an interpositional tissue and prevents bone-to-bone contact between the tuberosity and acromion.
© 2021 by the Arthroscopy Association of North America. Published by Elsevier.
Figures



References
-
- Burkhart S.S. Fluoroscopic comparison of kinematic patterns in massive rotator cuff tears. A suspension bridge model. Clin Orthop Relat Res. 1992:144–152. - PubMed
-
- Ecklund K.J., Lee T.Q., Tibone J., Gupta R. Rotator cuff tear arthropathy. J Am Acad Orthop Surg. 2007;15:340–349. - PubMed
-
- Green A. Chronic massive rotator cuff tears: Evaluation and management. J Am Acad Orthop Surg. 2003;11:321–331. - PubMed
-
- Mihata T., McGarry M.H., Pirolo J.M., Kinoshita M., Lee T.Q. Superior capsule reconstruction to restore superior stability in irreparable rotator cuff tears: A biomechanical cadaveric study. Am J Sports Med. 2012;40:2248–2255. - PubMed
-
- Lobao MH, Melvani RT, Abbasi P, Parks BG, Murthi AM. Dermal allograft superior capsule reconstruction biomechanics and kinematics [published online January 19, 2021]. J Shoulder Elbow Surg.https://doi.org/10.1016/j.jse.2020.11.024. - DOI - PubMed
LinkOut - more resources
Full Text Sources
