

Supply and Distribution of Vascular Access Physicians in the United States: A Cross-Sectional Study
- PMID: 34355198
- PMCID: PMC8336638
- DOI: 10.34067/kid.0002722020
Supply and Distribution of Vascular Access Physicians in the United States: A Cross-Sectional Study
Abstract
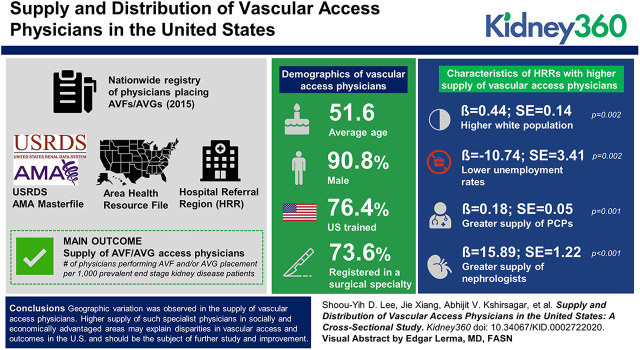
Background: Because functioning permanent vascular access (arteriovenous fistula [AVF] or arteriovenous graft [AVG]) is crucial for optimizing patient outcomes for those on hemodialysis, the supply of physicians placing vascular access is key. We investigated whether area-level demographic and healthcare market attributes were associated with the distribution and supply of AVF/AVG access physicians in the United States.
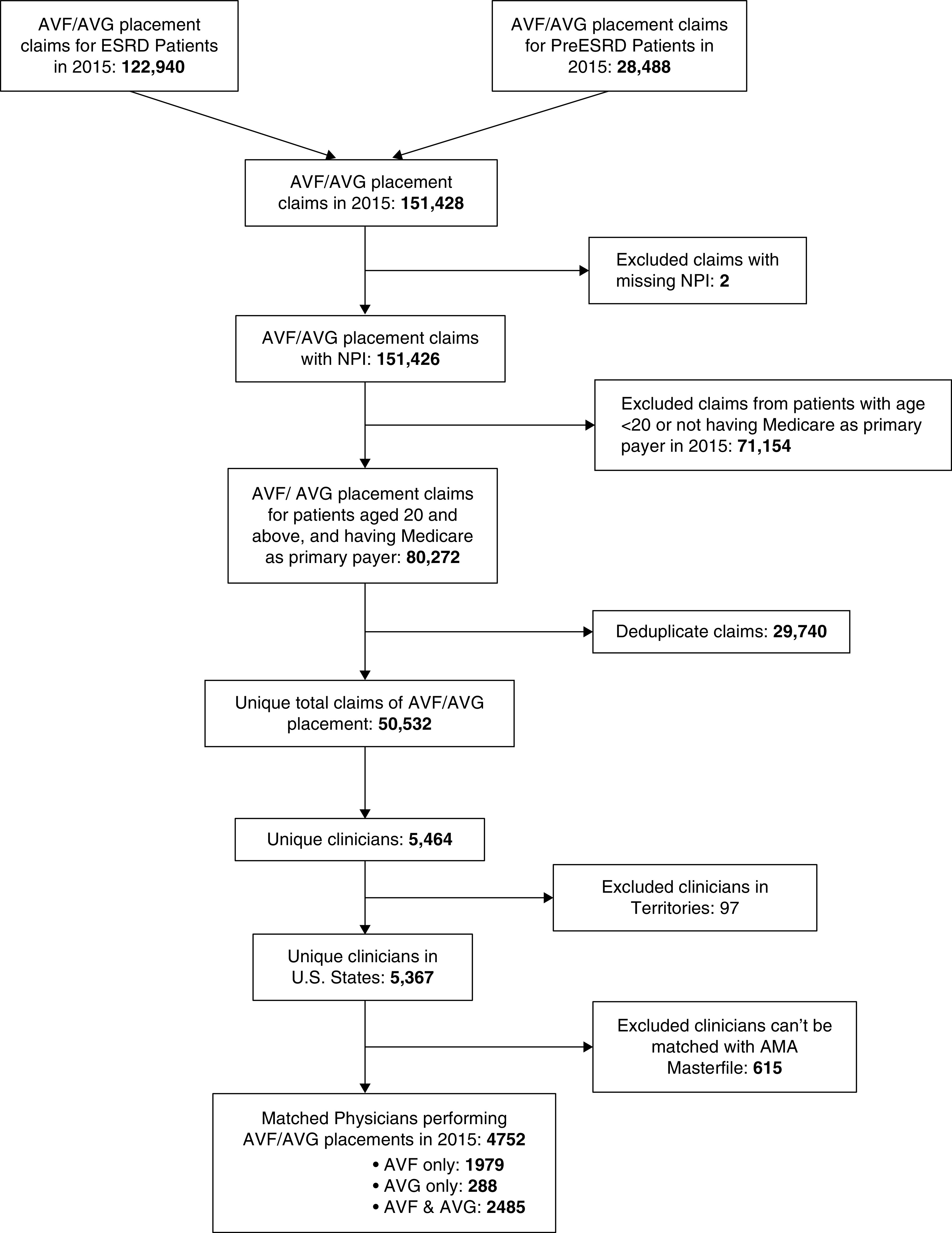
Methods: A nationwide registry of physicians placing AVFs/AVGs in 2015 was created using data from the United States Renal Data System and the American Physician Association's Physician Masterfile. We linked the registry information to the Area Health Resource File to assess the supply of AVF/AVG access physicians and their professional attributes by hospital referral region (HRR). Bivariate analysis and Poisson regression were performed to examine the relationship between AVF/AVG access physician supply and demographic, socioeconomic, and health resource conditions of HRRs. The setting included all 50 states. The main outcome was supply of AVF/AVG access physicians, defined as the number of physicians performing AVF and/or AVG placement per 1000 prevalent patients with ESKD.
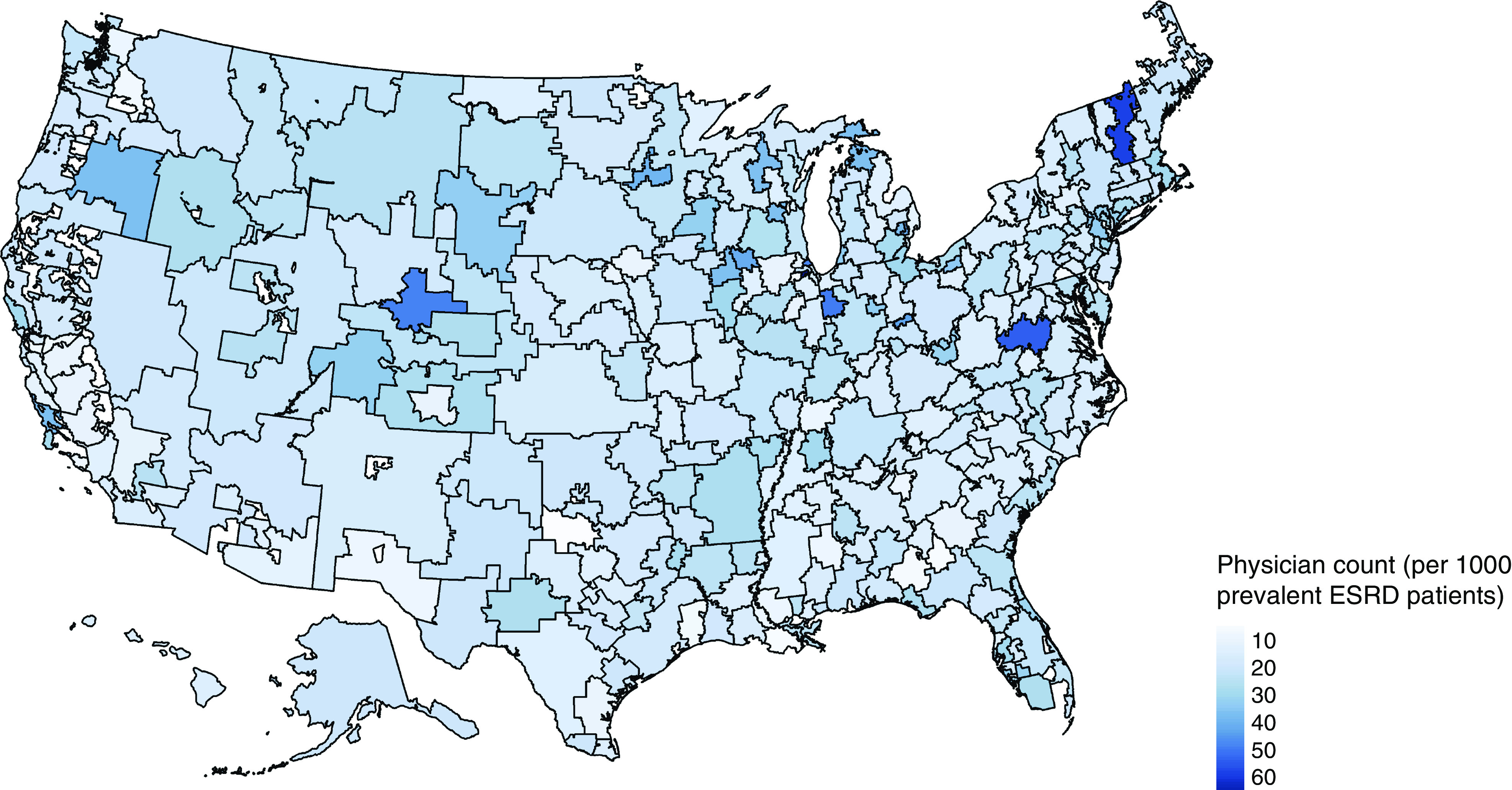
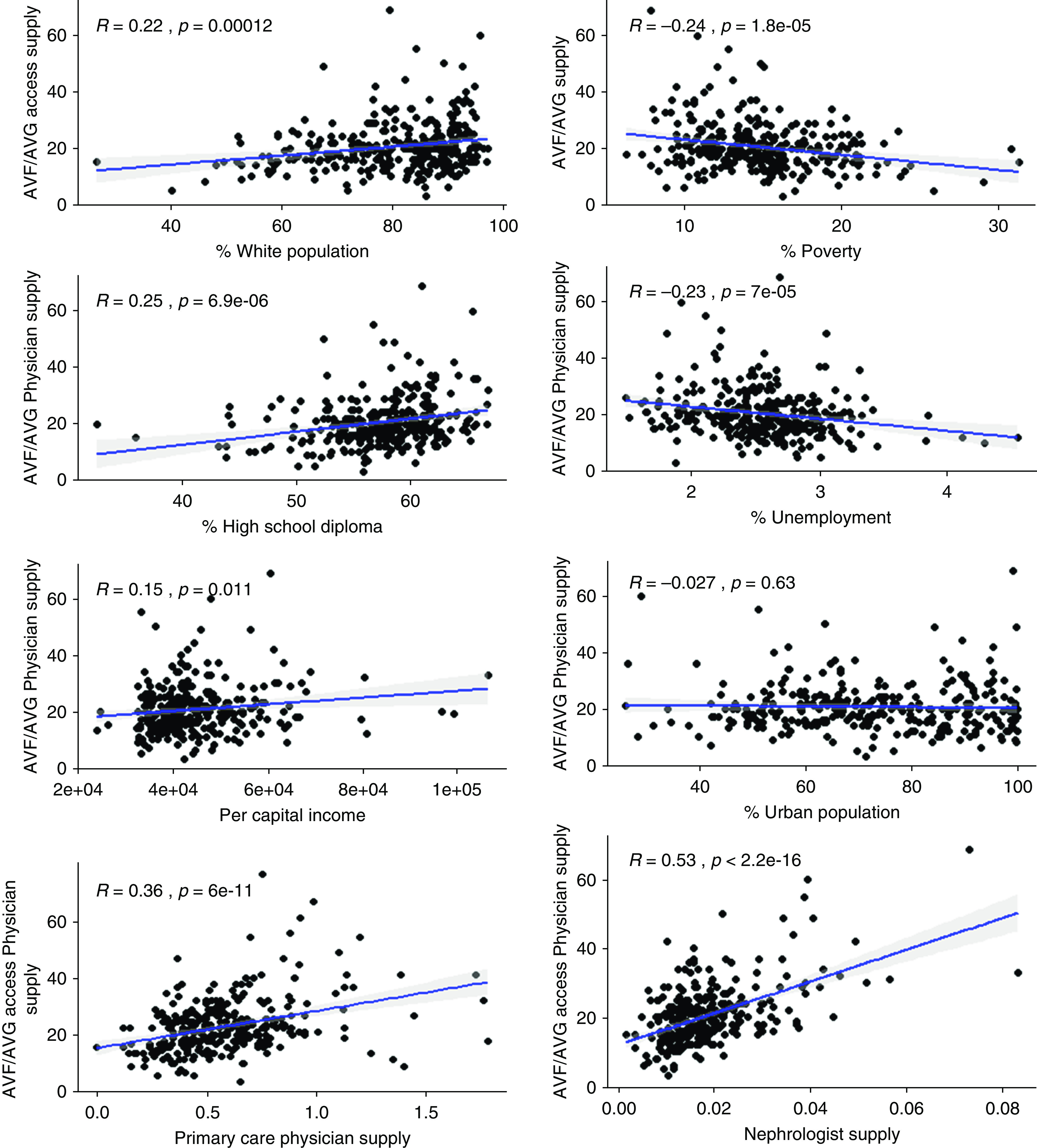
Results: The majority of vascular access physicians were aged 45-64 (average age, 51.6), male (91%), trained in the United States (76%), and registered in a surgical specialty (74%). The supply of physicians varied substantially across HRRs. The supply was higher in HRRs with a higher percentage white population (β=0.44; SEM=0.14; P=0.002), lower unemployment rates (β=-10.74; SEM=3.41; P=0.002), and greater supply of primary care physicians (β=0.18; SEM=0.05; P=0.001) and nephrologists (β=15.89; SEM=1.22; P<0.001).
Conclusions: Geographic variation was observed in the supply of vascular access physicians. Higher supply of such specialist physicians in socially and economically advantaged areas may explain disparities in vascular access and outcomes in the United States and should be the subject of further study and improvement.
Conflict of interest statement
All authors have nothing to disclose.
Figures
References
-
- Nassar GM, Ayus JC: Infectious complications of the hemodialysis access. Kidney Int 60: 1–13, 2001 - PubMed
-
- Fokou M, Teyang A, Ashuntantang G, Kaze F, Eyenga VC, Chichom Mefire A, Angwafo F 3rd: Complications of arteriovenous fistula for hemodialysis: An 8-year study. Ann Vasc Surg 26: 680–684, 2012 - PubMed
-
- Thamer M, Lee TC, Wasse H, Glickman MH, Qian J, Gottlieb D, Toner S, Pflederer TA: Medicare costs associated with arteriovenous fistulas among US hemodialysis patients. Am J Kidney Dis 72: 10–18, 2018 - PubMed
-
- Tokars JI, Light P, Anderson J, Miller ER, Parrish J, Armistead N, Jarvis WR, Gehr T: A prospective study of vascular access infections at seven outpatient hemodialysis centers. Am J Kidney Dis 37: 1232–1240, 2001 - PubMed
-
- Dhingra RK, Young EW, Hulbert-Shearon TE, Leavey SF, Port FK: Type of vascular access and mortality in U.S. hemodialysis patients. Kidney Int 60: 1443–1451, 2001 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
