

Antibiotic prophylaxis and the gastrointestinal resistome in paediatric patients with acute lymphoblastic leukaemia: a cohort study with metagenomic sequencing analysis
- PMID: 34355208
- PMCID: PMC8336918
- DOI: 10.1016/s2666-5247(20)30202-0
Antibiotic prophylaxis and the gastrointestinal resistome in paediatric patients with acute lymphoblastic leukaemia: a cohort study with metagenomic sequencing analysis
Abstract
Background: Although antibiotic prophylaxis with levofloxacin can reduce the risk of serious infection in immunocompromised patients, the potential contribution of prophylaxis to antibiotic resistance is a major drawback. We aimed to identify the effects of levofloxacin prophylaxis, given to paediatric patients with acute lymphoblastic leukaemia to prevent infections during induction chemotherapy, on antibiotic resistance in gastrointestinal microbiota after completion of induction and consolidation therapy.
Methods: This prospective, single-centre (St Jude Children's Research Hospital, Memphis, TN, USA) cohort study included children (≤18 years) receiving therapy for newly diagnosed acute lymphoblastic leukaemia and who received either primary levofloxacin prophylaxis or no antibacterial prophylaxis (aside from Pneumocystis jirovecii prophylaxis with trimethoprim-sulfamethoxazole) and provided at least two stool samples, including one after completion of induction therapy. We used metagenomic sequencing to identify bacterial genes that confer resistance to fluoroquinolones, trimethoprim-sulfamethoxazole, or other antibiotics, and to identify point mutations in bacterial topoisomerases (gyrA, parC) that confer resistance to fluoroquinolones. We then used generalised linear mixed models to compare the prevalence and relative abundance of antibiotic resistance gene groups after completion of induction and consolidation therapy between participants who had received levofloxacin and those who received no prophylaxis.
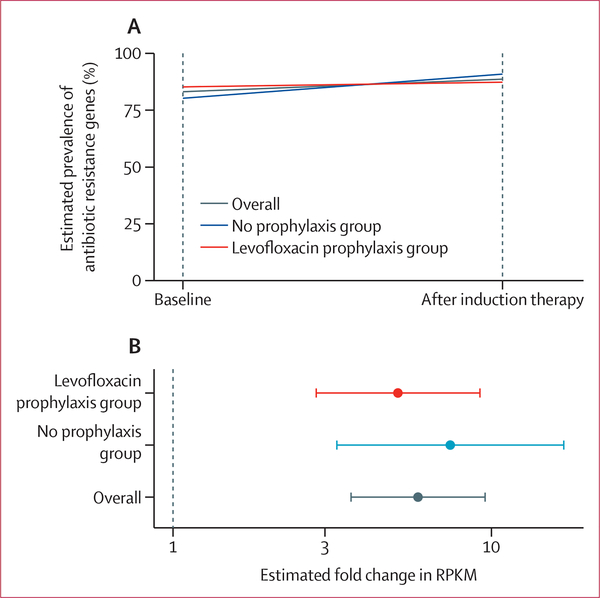
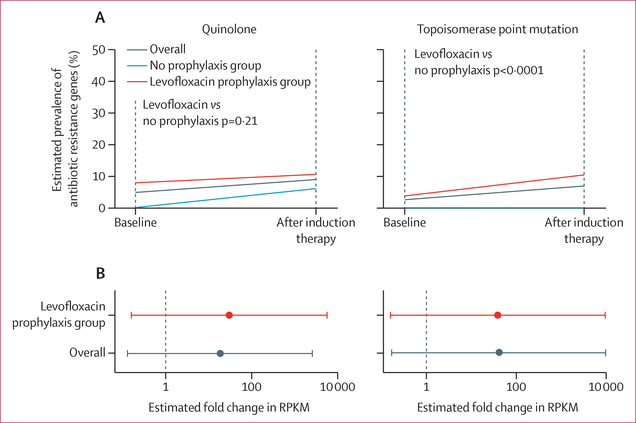
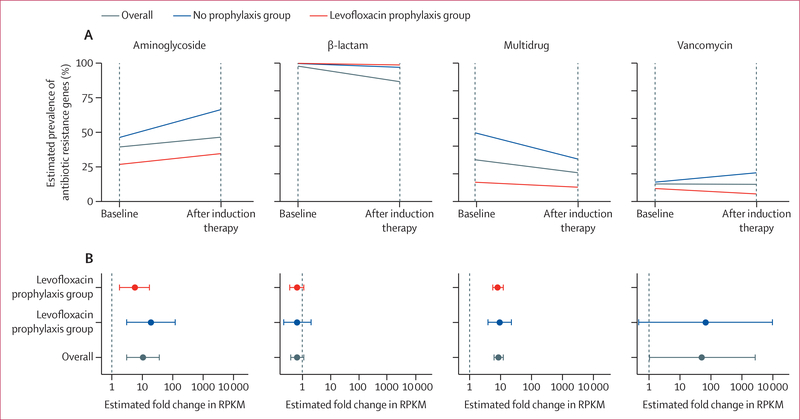
Findings: Between Feb 1, 2012, and April 30, 2016, 118 stool samples (32 baseline, 49 after induction, and 37 after consolidation) were collected from 49 evaluable participants; of these participants, 31 (63%) received levofloxacin prophylaxis during induction therapy and 18 (37%) received no antibacterial prophylaxis. Over the course of induction therapy, there was an overall increase in the relative abundance of trimethoprim-sulfamethoxazole resistance genes (estimated mean fold change 5·9, 95% CI 3·6-9·6; p<0·0001), which was not modified by levofloxacin prophylaxis (p=0·46). By contrast, the prevalence of topoisomerase point mutations increased over the course of induction therapy in levofloxacin recipients (mean prevalence 10·4% [95% CI 3·2-25·4] after induction therapy vs 3·7% [0·2-22·5] at baseline) but not other participants (0% vs 0%; p<0·0001). There was no significant difference between prophylaxis groups with respect to changes in aminoglycoside, β-lactam, vancomycin, or multidrug resistance genes after completion of induction or consolidation therapy.
Interpretation: Analysing the gastrointestinal resistome can provide insights into the effects of antibiotics on the risk of antibiotic-resistant infections. In this study, antibiotic prophylaxis with trimethoprim-sulfamethoxazole or levofloxacin during induction therapy for acute lymphoblastic leukaemia appeared to increase the short-term and medium-term risk of colonisation with bacteria resistant to these antibiotics, but not to other drugs. More research is needed to determine the longer-term effects of antibacterial prophylaxis on colonisation with antibiotic-resistant bacteria.
Funding: Children's Infection Defense Center at St Jude Children's Research Hospital, American Lebanese Syrian Associated Charities, and National Institutes of Health.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Similar articles
-
Levofloxacin Prophylaxis During Induction Therapy for Pediatric Acute Lymphoblastic Leukemia.Clin Infect Dis. 2017 Nov 13;65(11):1790-1798. doi: 10.1093/cid/cix644. Clin Infect Dis. 2017. PMID: 29020310 Free PMC article. Clinical Trial.
-
Prophylactic Use Of Levofloxacin During Induction Of Acute Lymphoblastic Leukaemia In Children-Experience From Pakistan.J Pak Med Assoc. 2023 Oct;73(10):2065-2068. doi: 10.47391/JPMA.7383. J Pak Med Assoc. 2023. PMID: 37876072
-
Effect of Levofloxacin Prophylaxis on Bacteremia in Children With Acute Leukemia or Undergoing Hematopoietic Stem Cell Transplantation: A Randomized Clinical Trial.JAMA. 2018 Sep 11;320(10):995-1004. doi: 10.1001/jama.2018.12512. JAMA. 2018. PMID: 30208456 Free PMC article. Clinical Trial.
-
Fluoroquinolone Prophylaxis in Children With Cancer: A Pro/Con Discussion.J Pediatric Infect Dis Soc. 2024 Sep 26;13(9):486-492. doi: 10.1093/jpids/piae077. J Pediatric Infect Dis Soc. 2024. PMID: 39073450 Review.
-
Fluoroquinolones versus trimethoprim-sulfamethoxazole for the treatment of Stenotrophomonas maltophilia infections: a systematic review and meta-analysis.Clin Microbiol Infect. 2019 May;25(5):546-554. doi: 10.1016/j.cmi.2018.11.008. Epub 2018 Nov 16. Clin Microbiol Infect. 2019. PMID: 30448331
Cited by
-
Fluoroquinolone Use Among Hospitalized Children: Diagnosis-Based Stratification to Identify Stewardship Targets.Open Forum Infect Dis. 2023 May 29;10(6):ofad297. doi: 10.1093/ofid/ofad297. eCollection 2023 Jun. Open Forum Infect Dis. 2023. PMID: 37323425 Free PMC article.
-
Effectiveness of Quinolone Prophylaxis in Pediatric Acute Leukemia and Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-analysis.Open Forum Infect Dis. 2022 Nov 3;9(12):ofac594. doi: 10.1093/ofid/ofac594. eCollection 2022 Dec. Open Forum Infect Dis. 2022. PMID: 36504701 Free PMC article. Review.
-
Prevention and Management of Infectious Complications in Pediatric Patients With Cancer: A Survey Assessment of Current Practices Across Children's Oncology Group Institutions.Pediatr Blood Cancer. 2025 Mar;72(3):e31532. doi: 10.1002/pbc.31532. Epub 2025 Jan 8. Pediatr Blood Cancer. 2025. PMID: 39780366
-
The gastrointestinal antibiotic resistome in pediatric leukemia and lymphoma patients.Front Cell Infect Microbiol. 2023 Feb 24;13:1102501. doi: 10.3389/fcimb.2023.1102501. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 36909730 Free PMC article.
-
The effects of antibiotic exposures on the gut resistome during hematopoietic cell transplantation in children.Gut Microbes. 2024 Jan-Dec;16(1):2333748. doi: 10.1080/19490976.2024.2333748. Epub 2024 Mar 30. Gut Microbes. 2024. PMID: 38555499 Free PMC article.
References
-
- O’Connor D, Bate J, Wade R, et al. Infection-related mortality in children with acute lymphoblastic leukemia: an analysis of infectious deaths on UKALL2003. Blood 2014; 124: 1056–61. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous