

Predictors of Lack of Relapse After Random Discontinuation of Oral and Long-acting Injectable Antipsychotics in Clinically Stabilized Patients with Schizophrenia: A Re-analysis of Individual Participant Data
- PMID: 34355232
- PMCID: PMC8886604
- DOI: 10.1093/schbul/sbab091
Predictors of Lack of Relapse After Random Discontinuation of Oral and Long-acting Injectable Antipsychotics in Clinically Stabilized Patients with Schizophrenia: A Re-analysis of Individual Participant Data
Abstract
Objective: To quantify the risk and predictors of relapse among individuals with schizophrenia randomly withdrawn from antipsychotic maintenance treatment.
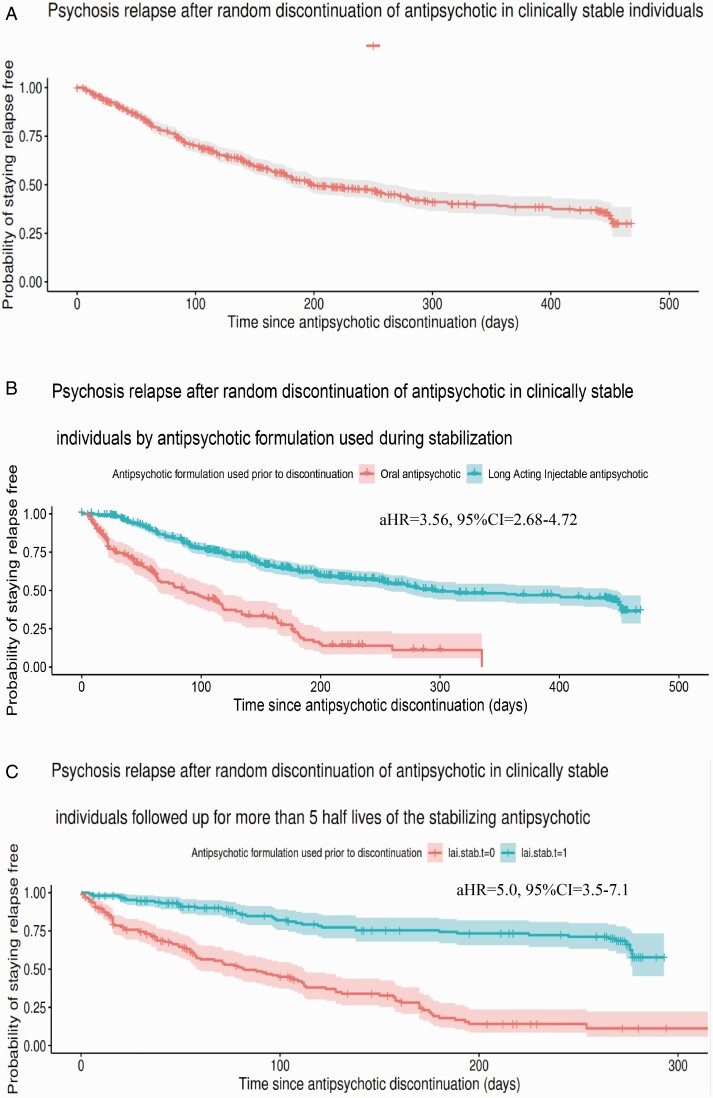
Methods: We re-analyzed time-to-event and baseline predictors from placebo arms in five placebo-controlled randomized trials of antipsychotics (n = 688 individuals; 173 stabilized on oral antipsychotic [OAP] and 515 on long-acting injectables [LAI]) for relapse-prevention available in the Yale Open Data Access repository. Using a survival and Cox-proportional hazards regression analyses, we estimated survival rates of "relapse-free" individuals by the end of follow-up (median = 118 days, IQR = 52.0-208.0), the rate of study-confirmed relapse, and adjusted hazard ratios (aHR, 95% confidence intervals [CI]) associated with baseline predictors. We also estimated these parameters for individuals followed for >5 half-lives of the stabilizing antipsychotic, and studied predictors of "rebound psychosis" in OAP-stabilized participants, defined as occurring within 30 days of antipsychotic withdrawal.
Results: 29.9% (95%CI = 23.2-38.5) remained relapse-free by the end of follow-up, 11.1% (95%CI = 5.65-21.9) among those OAP-stabilized, 36.4% (95%CI = 28.4-46.7) among those LAI-stabilized. The study-confirmed relapse rate was 45.2%, 62.4% among those OAP-stabilized and 39.4% among those LAI-stabilized. Predictors of relapse included smoking (aHR = 1.54, 95%CI = 1.19-2.00), female sex (aHR = 1.37, 95%CI = 1.08-1.79), and having been stabilized on OAPs vs LAIs (aHR = 3.56, 95%CI = 2.68-4.72). Greater risk of relapse on OAP persisted even after sufficient time had elapsed to clear antipsychotic plasma level among LAI-stabilized (aHR = 5.0, 95%CI = 3.5-7.1). "Rebound psychosis" did not show predictors.
Conclusions and relevance: Our results corroborate the high relapse risk following antipsychotic withdrawal after symptom stabilization with limited patient-related predictors of safe treatment discontinuation. Stabilization with LAIs reduces the short-/medium-term relapse risk.
Keywords: antipsychotics; individual participant data; long-acting injectables; relapse; schizophrenia; withdrawal.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Confounding of Antipsychotic Discontinuation Studies by Withdrawal-Related Relapse.Schizophr Bull. 2022 Mar 1;48(2):294-295. doi: 10.1093/schbul/sbab146. Schizophr Bull. 2022. PMID: 34964477 Free PMC article. No abstract available.
References
-
- Millan MJ, Andrieux A, Bartzokis G, et al. . Altering the course of schizophrenia: progress and perspectives. Nat Rev Drug Discov. 2016;15(7):485–515. - PubMed
-
- Almond S, Knapp M, Francois C, Toumi M, Brugha T. Relapse in schizophrenia: costs, clinical outcomes and quality of life. Br J Psychiatry. 2004;184:346–351. - PubMed
-
- Emsley R, Chiliza B, Asmal L. The evidence for illness progression after relapse in schizophrenia. Schizophr Res. 2013;148(1-3):117–121. - PubMed
-
- Mayoral-van Son J, de la Foz VO, Martinez-Garcia O, et al. . Clinical outcome after antipsychotic treatment discontinuation in functionally recovered first-episode nonaffective psychosis individuals: a 3-year naturalistic follow-up study. J Clin Psychiatry. 2016;77(4):492–500. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
