

Evidence, not eminence, for surgical management during COVID-19: a multifaceted systematic review and a model for rapid clinical change
- PMID: 34355242
- PMCID: PMC8342932
- DOI: 10.1093/bjsopen/zrab048
Evidence, not eminence, for surgical management during COVID-19: a multifaceted systematic review and a model for rapid clinical change
Abstract
Background: Coronavirus (COVID-19) forced surgical evolution worldwide. The extent to which national evidence-based recommendations, produced by the current authors early in 2020, remain valid, is unclear. To inform global surgical management and a model for rapid clinical change, this study aimed to characterize surgical evolution following COVID-19 through a multifaceted systematic review.
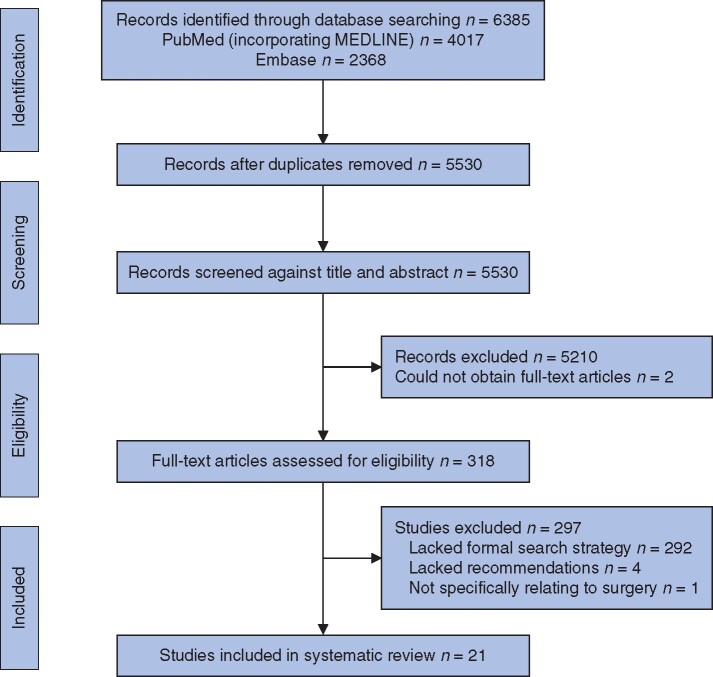
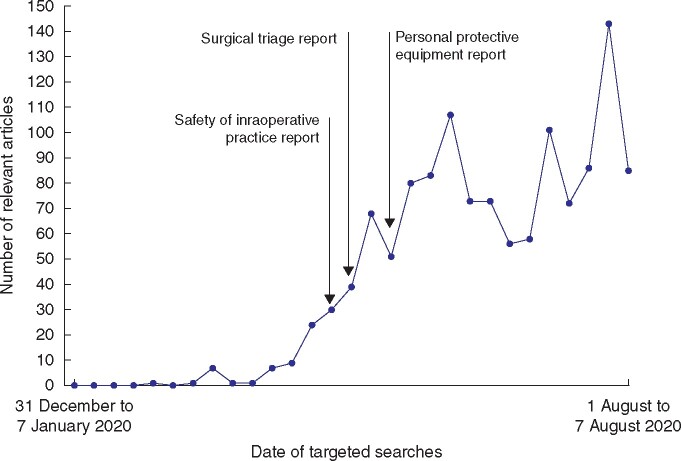
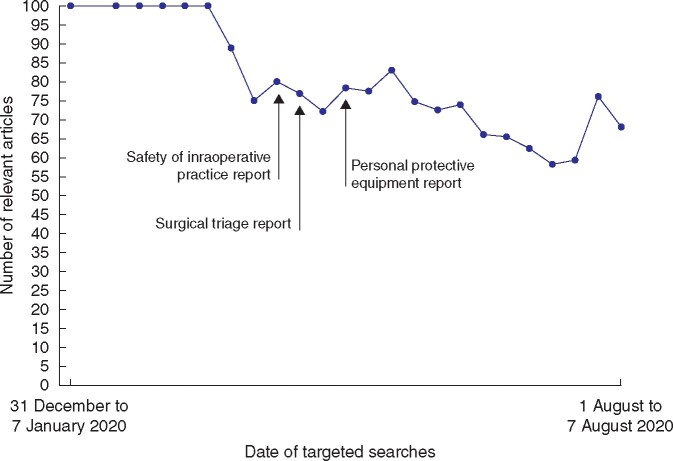
Methods: Rapid reviews were conducted targeting intraoperative safety, personal protective equipment and triage, alongside a conventional systematic review identifying evidence-based guidance for surgical management. Targeted searches of PubMed and Embase from 31 December 2019 were repeated weekly until 7 August 2020, and systematic searches repeated monthly until 30 June 2020. Literature was stratified using Evans' hierarchy of evidence. Narrative data were analysed for consistency with earlier recommendations. The systematic review rated quality using the AGREE II and AMSTAR tools, was registered with PROSPERO, CRD42020205845. Meta-analysis was not conducted.
Results: From 174 targeted searches and six systematic searches, 1256 studies were identified for the rapid reviews and 21 for the conventional systematic review. Of studies within the rapid reviews, 903 (71.9 per cent) had lower-quality design, with 402 (32.0 per cent) being opinion-based. Quality of studies in the systematic review ranged from low to moderate. Consistency with recommendations made previously by the present authors was observed despite 1017 relevant subsequent publications.
Conclusion: The evidence-based recommendations produced early in 2020 remained valid despite many subsequent publications. Weaker studies predominated and few guidelines were evidence-based. Extracted clinical solutions were globally implementable. An evidence-based model for rapid clinical change is provided that may benefit surgical management during this pandemic and future times of urgency.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Kibbe MR. Surgery and COVID-19. JAMA 2020;324:1151–1152 - PubMed
-
- Zarzaur BL, Stahl CC, Greenberg JA, Savage SA, Minter RM.. Blueprint for restructuring a department of surgery in concert with the health care system during a pandemic: The University of Wisconsin Experience. JAMA Surg 2020;155:628–635 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
