

Nasal endoscopy, room filtration, and aerosol concentrations during live outpatient encounters: a prospective, case-control study
- PMID: 34355871
- PMCID: PMC8427097
- DOI: 10.1002/alr.22874
Nasal endoscopy, room filtration, and aerosol concentrations during live outpatient encounters: a prospective, case-control study
Abstract
Background: The coronavirus disease 2019 (COVID-19) pandemic has highlighted safety concerns surrounding possible aerosol-generating procedures, but comparative data on the smallest particles capable of transmitting this virus remain limited. We evaluated the effect of nasal endoscopy on aerosol concentration and the role of a high-efficiency particulate air (HEPA) filter in reducing aerosol concentration.
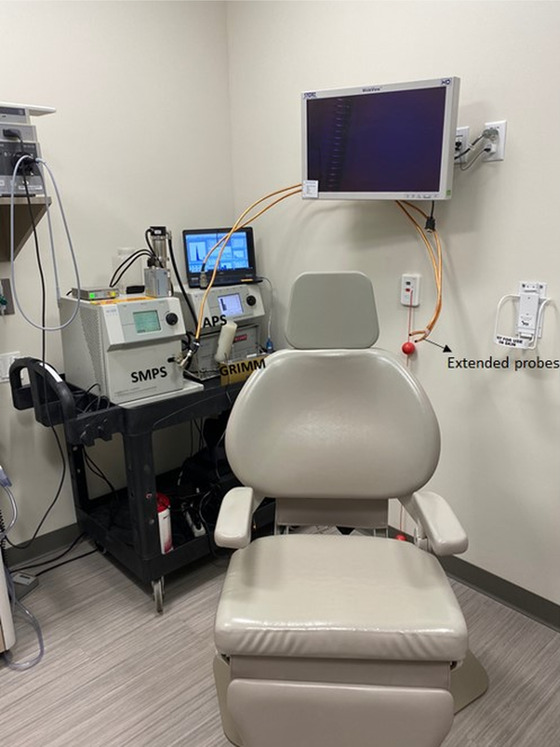
Methods: Otolaryngology patients were prospectively enrolled in an outpatient, cross-sectional study. Demographic information and clinic room characteristics were recorded. A scanning mobility particle sizer and GRIMM aerosol monitor measured aerosols 14.3 nm to 34 μm in diameter (i.e., particles smaller than those currently examined in the literature) during (1) nasal endoscopy (± debridement) and (2) no nasal endoscopy encounters. One-way analysis of variance (ANOVA) and Student's t test were performed to compare aerosol concentrations and impact of HEPA filtration.
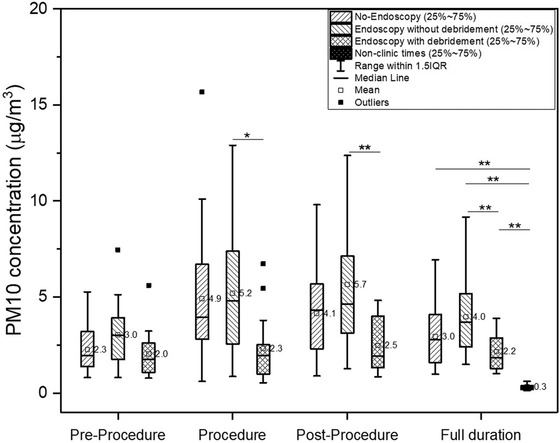
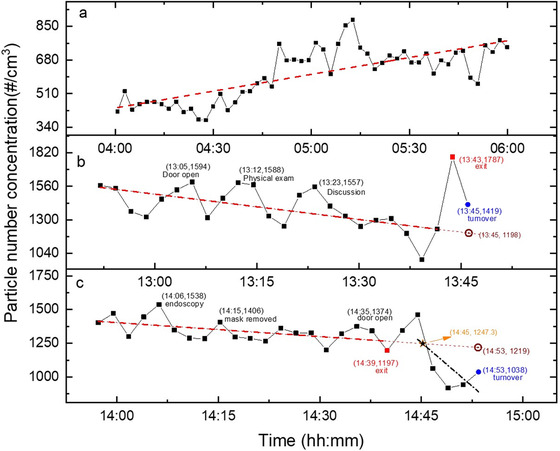
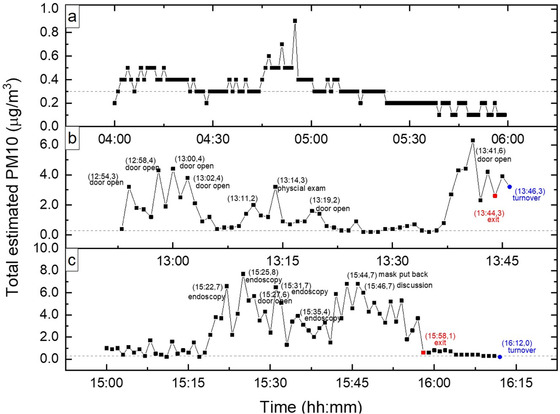
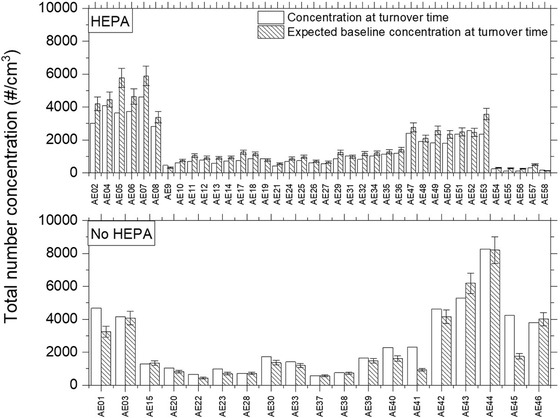
Results: Sixty-two patients met inclusion criteria (25 nasal endoscopy without debridement; 18 nasal endoscopy with debridement; 19 no nasal endoscopy). There was no significant difference in age or gender across cohorts. Aerosol concentration in the nasal endoscopy cohort (± debridement) was not greater than the no nasal endoscopy cohort (p = 0.36; confidence interval [95% CI], -1.76 to 0.17 μg/m3 ; and p = 0.12; 95% CI, -0.11 to 2.14 μg/m3 , respectively). Aerosol concentrations returned to baseline after 8.76 min without a HEPA filter versus 4.75 min with a HEPA filter (p = 0.001; 95% CI, 1.73-6.3 min).
Conclusion: Using advanced instrumentation and a comparative study design, aerosol concentration was shown to be no greater during nasal endoscopy versus no endoscopy encounters. HEPA filter utilization reduced aerosol concentrations significantly faster than no HEPA filter.
Keywords: COVID-19; aerosol; filter; nasal endoscopy; otolaryngology.
© 2021 ARS-AAOA, LLC.
Conflict of interest statement
Jeremiah A. Alt: OptiNose, GlycoMira, Medtronic, and GSK. Kerry Kelly: Tetrad.
Figures
References
-
- Centers for Disease Control and Prevention (CDC) . Clinical questions about COVID‐19: questions and answers. Atlanta, GA: CDC; March 2021. https://www.cdc.gov/coronavirus/2019‐ncov/hcp/faq.html. Accessed July 22, 2021.
-
- World Health Organization (WHO) . Infection prevention and control of epidemic‐ and pandemic‐prone acute respiratory infections in health care. Geneva: WHO; 2014. https://www.who.int/publications/i/item/infection‐prevention‐and‐control.... Accessed July 22, 2021. - PubMed
-
- Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Healthcare Quality Promotion (DHQP) . Appendix B. Air. Guidelines for Environmental Infection Control in Health‐Care Facilities (2003). Atlanta, GA: CDC; Page last reviewed July 22, 2019. https://www.cdc.gov/infectioncontrol/guidelines/environmental/appendix/a.... Accessed July 22, 2021.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
