

Occluded Superior Mesenteric Artery and Vein. Therapy with the Stable Gastric Pentadecapeptide BPC 157
- PMID: 34356860
- PMCID: PMC8301404
- DOI: 10.3390/biomedicines9070792
Occluded Superior Mesenteric Artery and Vein. Therapy with the Stable Gastric Pentadecapeptide BPC 157
Abstract
Background: We investigated the occluded essential vessel tributaries, both arterial and venous, occluded superior mesenteric vein and artery in rats, consequent noxious syndrome, peripherally and centrally. As therapy, we hypothesized the rapidly activated alternative bypassing pathways, arterial and venous, and the stable gastric pentadecapeptide BPC 157 since it rapidly alleviated venous occlusion syndromes.
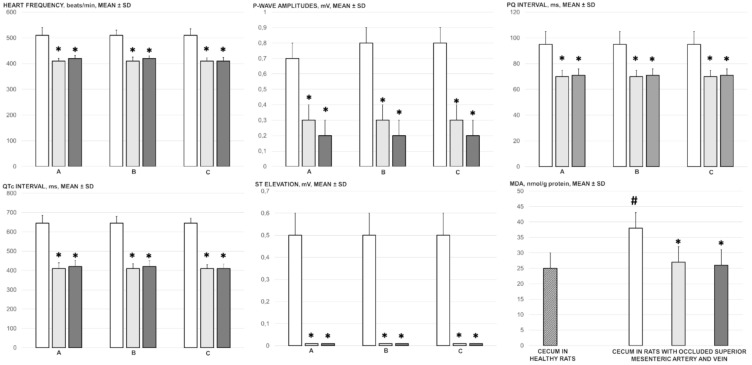
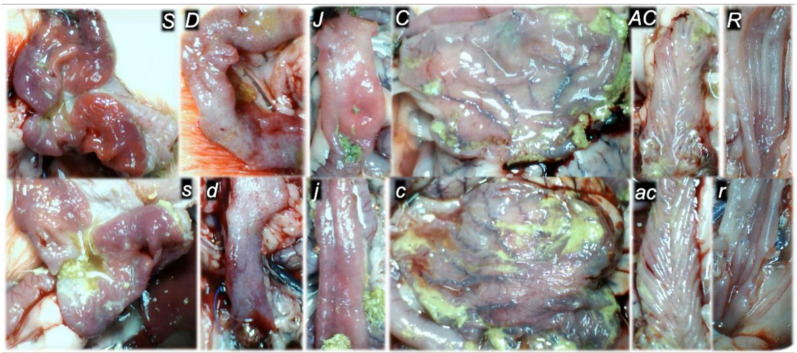
Methods: Assessments were performed for 30 min (gross recording, venography, ECG, pressure, microscopy, biochemistry, and oxidative stress), including portal hypertension, caval hypertension, aortal hypotension, and centrally, the superior sagittal sinus hypertension; systemic arterial and venous thrombosis, ECG disturbances, MDA-tissue increase, the multiple organs lesions, heart, lung, liver, kidney and gastrointestinal tract, including brain (swelling, and cortex (cerebral, cerebellar), hypothalamus/thalamus, hippocampus lesions). Rats received BPC 157 medication (10 µg/kg, 10 ng/kg) intraperitoneally at 1 min ligation-time.
Results: BPC 157 rapidly activated collateral pathways. These collateral loops were the superior mesenteric vein-inferior anterior pancreaticoduodenal vein-superior anterior pancreaticoduodenal vein-pyloric vein-portal vein pathway, an alternative pathway toward inferior caval vein via the united middle colic vein and inferior mesenteric vein through the left colic vein, and the inferior anterior pancreaticoduodenal artery and inferior mesenteric artery. Consequently, BPC 157 counteracted the superior sagittal sinus, portal and caval hypertension, aortal hypotension, progressing venous and arterial thrombosis peripherally and centrally, ECG disturbances attenuated. Markedly, the multiple organs lesions, heart, lung, liver, kidney, and gastrointestinal tract, in particular, as well as brain lesions, and oxidative stress in tissues were attenuated.
Conclusions: BPC 157 therapy rapidly recovered rats, which have complete occlusion of the superior mesenteric vein and artery.
Keywords: BPC 157; rats; superior mesenteric vein and artery occlusion; vascular recruitment.
Conflict of interest statement
The authors declare that there are no conflict of interest.
Figures












References
-
- Sikiric P., Rucman R., Turkovic B., Sever M., Klicek R., Radic B., Drmic D., Stupnisek M., Misic M., Vuletic L.B., et al. Novel cytoprotective mediator, stable gastric pentadecapeptide BPC 157. Vascular recruitment and gastrointestinal tract healing. Curr. Pharm. Des. 2018;24:1990–2001. doi: 10.2174/1381612824666180608101119. - DOI - PubMed
-
- Sikiric P., Hahm K.B., Blagaic A.B., Tvrdeic A., Pavlov K.H., Petrovic A., Kokot A., Gojkovic S., Krezic I., Drmic D., et al. Stable Gastric Pentadecapeptide BPC 157, Robert’s stomach cytoprotection/adaptive cytoprotection/organoprotection, and Selye’s stress coping response: Progress, achievements, and the future. Gut Liver. 2020;14:153–167. doi: 10.5009/gnl18490. - DOI - PMC - PubMed
-
- Vukojevic J., Siroglavic M., Kasnik K., Kralj T., Stancic D., Kokot A., Kolaric D., Drmic D., Sever A.Z., Barisic I., et al. Rat inferior caval vein (ICV) ligature and particular new insights with the stable gastric pentadecapeptide BPC 157. Vascul. Pharmacol. 2018;106:54–66. doi: 10.1016/j.vph.2018.02.010. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
