

High-Resolution CT Findings of Myositis-Related Interstitial Lung Disease
- PMID: 34356972
- PMCID: PMC8304263
- DOI: 10.3390/medicina57070692
High-Resolution CT Findings of Myositis-Related Interstitial Lung Disease
Abstract
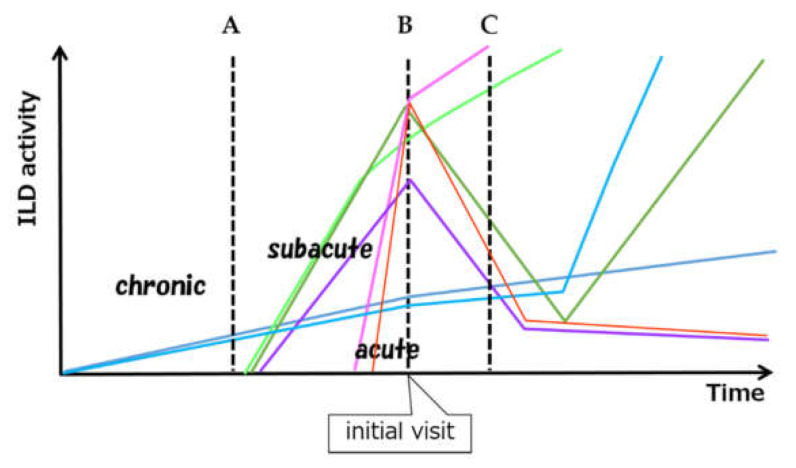
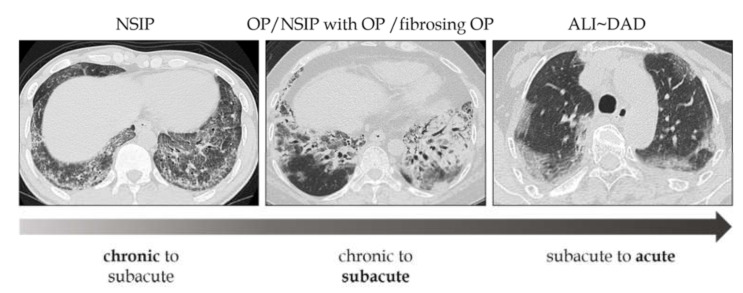
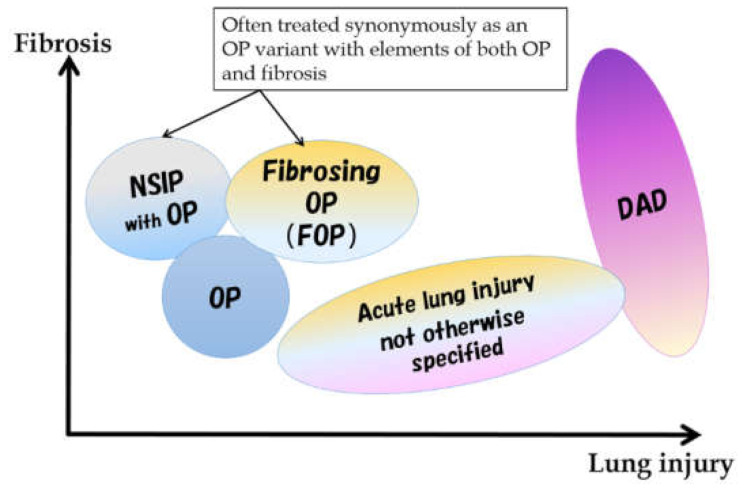
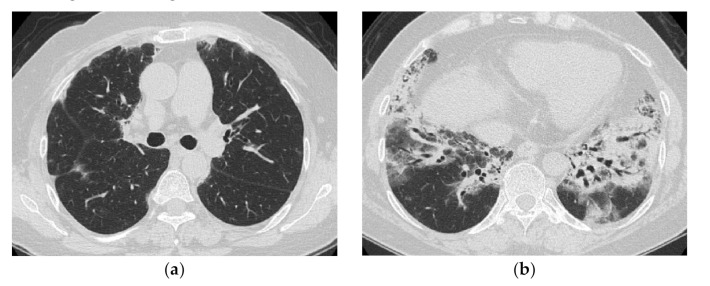
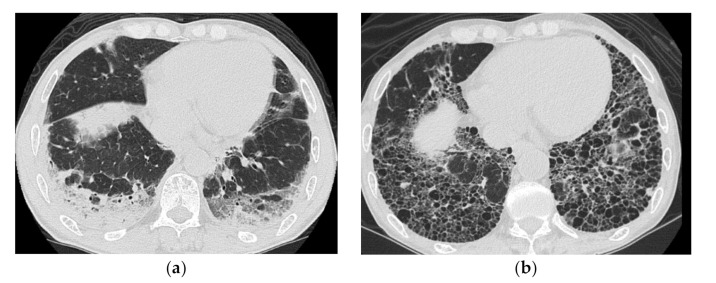
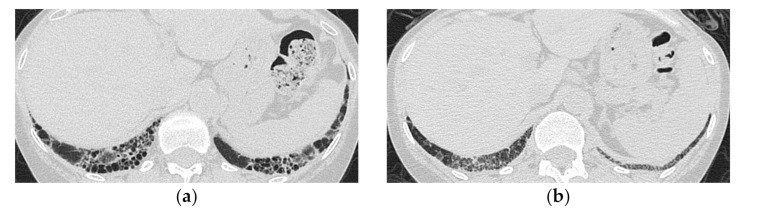
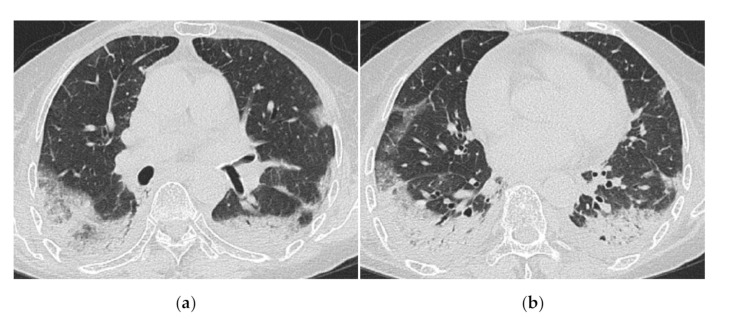
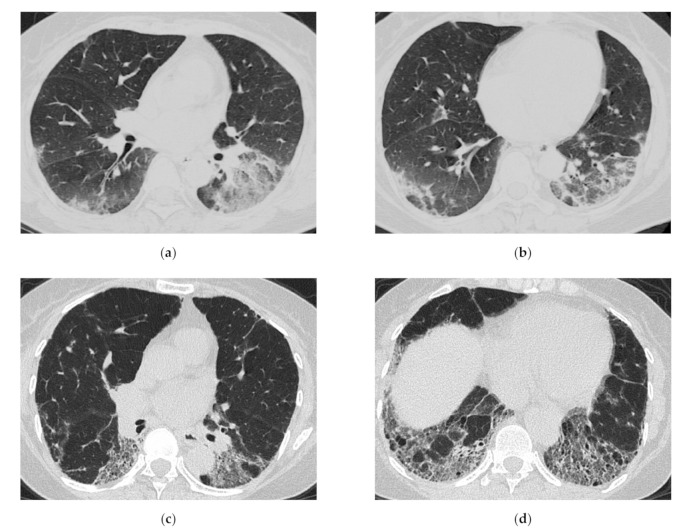
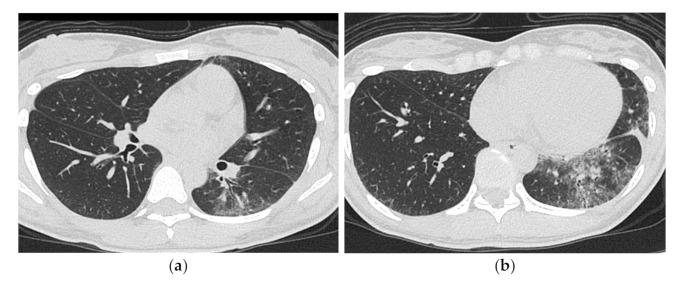
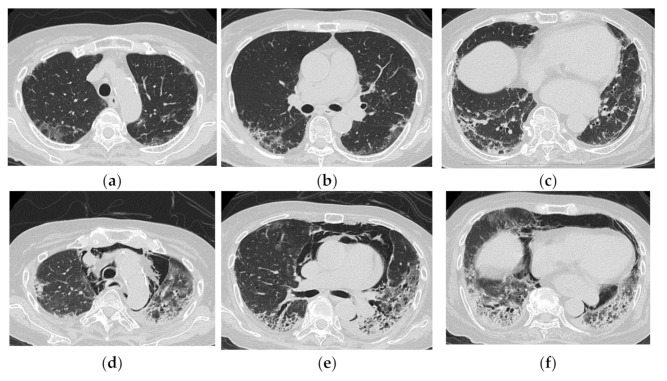
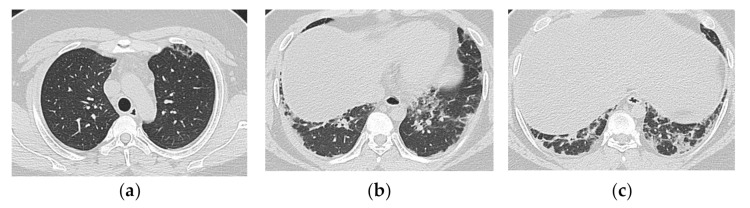
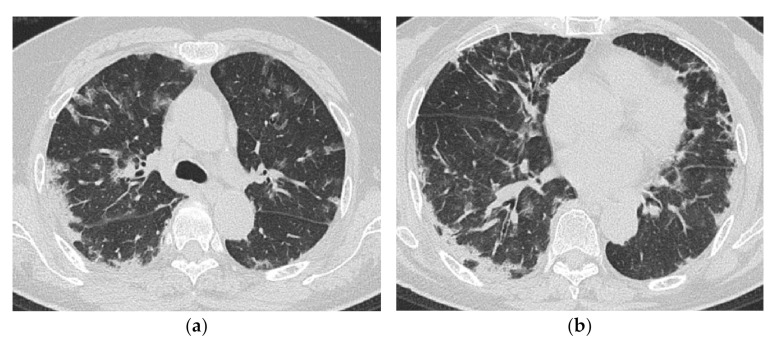
Myositis-related interstitial lung disease presents with a wide variety of lesions, ranging from chronic to acute. It can be divided into two main forms by the types of onsets, namely, chronic to subacute type showing nonspecific interstitial pneumonia (NSIP) or NSIP with an organizing pneumonia (OP)/fibrosing OP (FOP) pattern and acute type showing acute lung injury (ALI) to diffuse alveolar damage (DAD) pattern. Anti-aminoacyl tRNA Synthetase antibody-positive cases mainly show an NSIP or FOP pattern, whereas anti-melanoma differentiation-associated gene 5 antibody-positive cases show ALI to DAD pattern. Bilateral consolidation with or without ground-glass opacification with lower lobe predominance is common as a major pattern in all types, but the distribution or extent is sometimes different. The early detection of findings that indicate a rapid progressive course is vital. Diffuse cranio-caudal distribution and multiple ground-glass opacifications with random distribution might indicate a poorer prognosis.
Keywords: anti- synthetase syndrome; high-resolution CT; interstitial lung disease; interstitial pneumonia; myositis-specific antibody; polymyositis/dermatomyositis.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
-
- Travis W.D., Costabel U., Hansell D.M., King T.E., Jr., Lynch D.A., Nicholson A.G., Ryerson C.J., Ryu J.H., Selman M., Wells A.U., et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013;188:733–748. doi: 10.1164/rccm.201308-1483ST. - DOI - PMC - PubMed
-
- Fujisawa T., Suda T., Nakamura Y., Enomoto N., Ide K., Toyoshima M., Uchiyama H., Tamura R., Ida M., Yagi T., et al. Differences in clinical features and prognosis of interstitial lung diseases between polymyositis and dermatomyositis. J. Rheumatol. 2005;32:58–64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
