

Robotic Esophagectomy. A Systematic Review with Meta-Analysis of Clinical Outcomes
- PMID: 34357107
- PMCID: PMC8306060
- DOI: 10.3390/jpm11070640
Robotic Esophagectomy. A Systematic Review with Meta-Analysis of Clinical Outcomes
Abstract
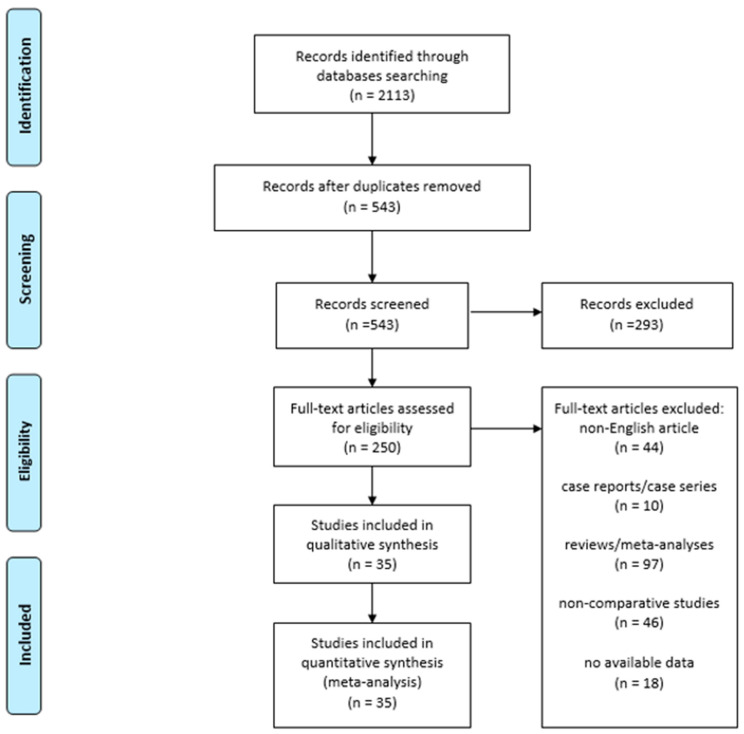
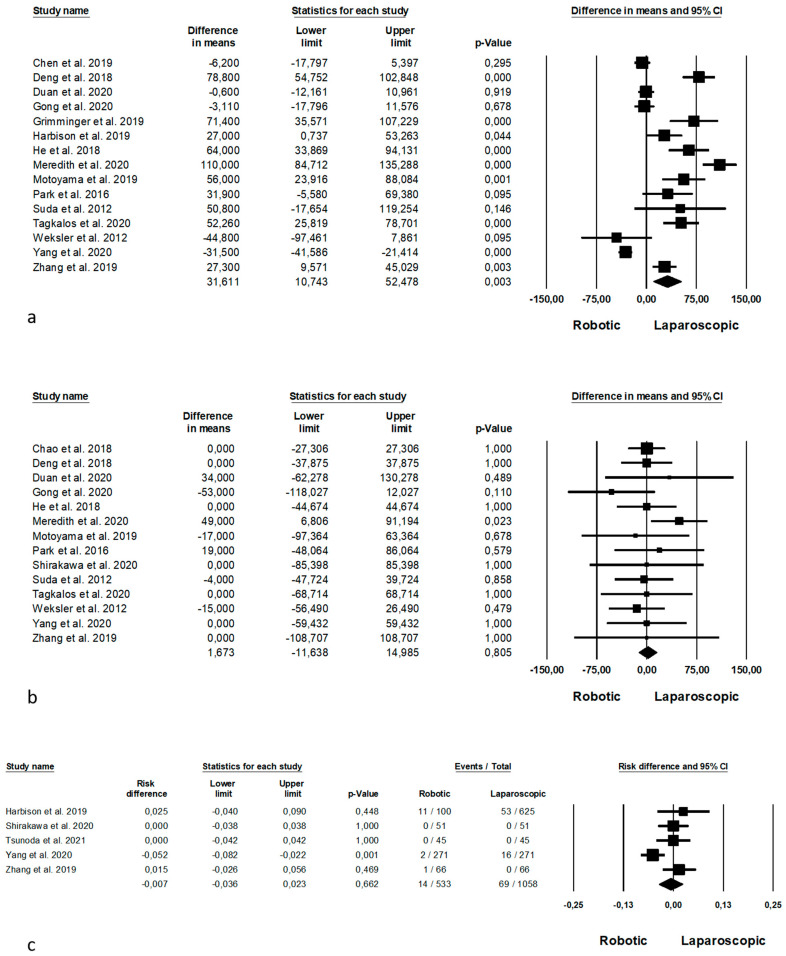
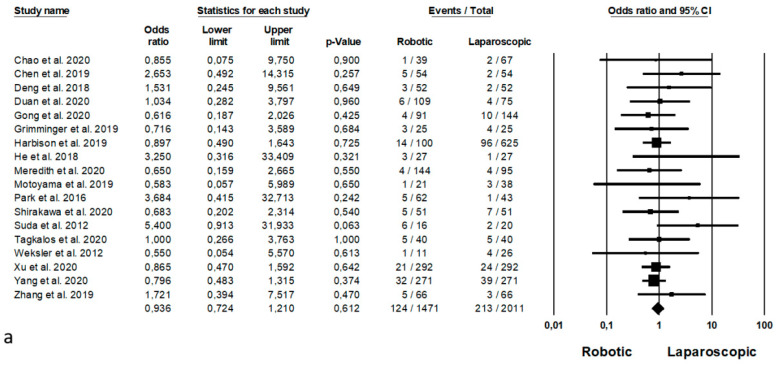
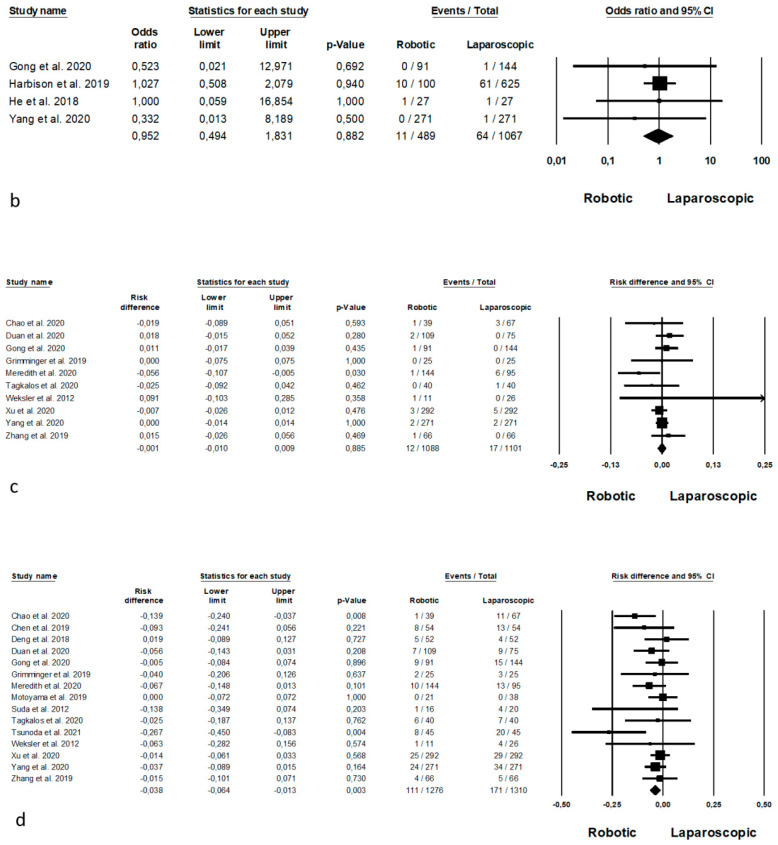
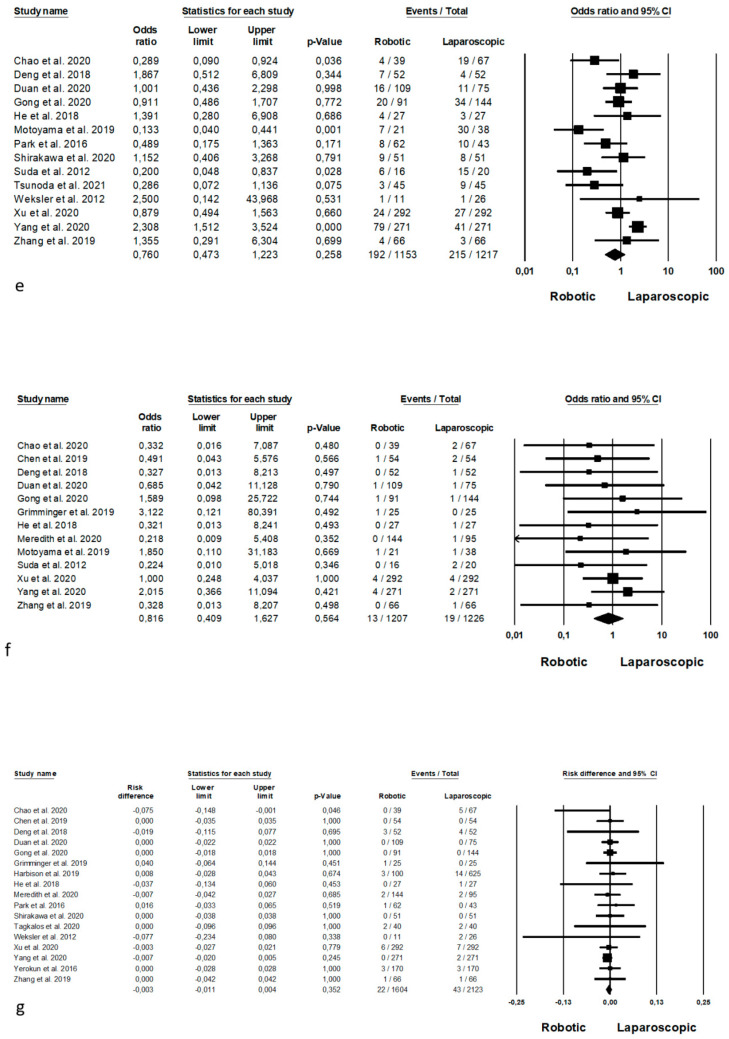
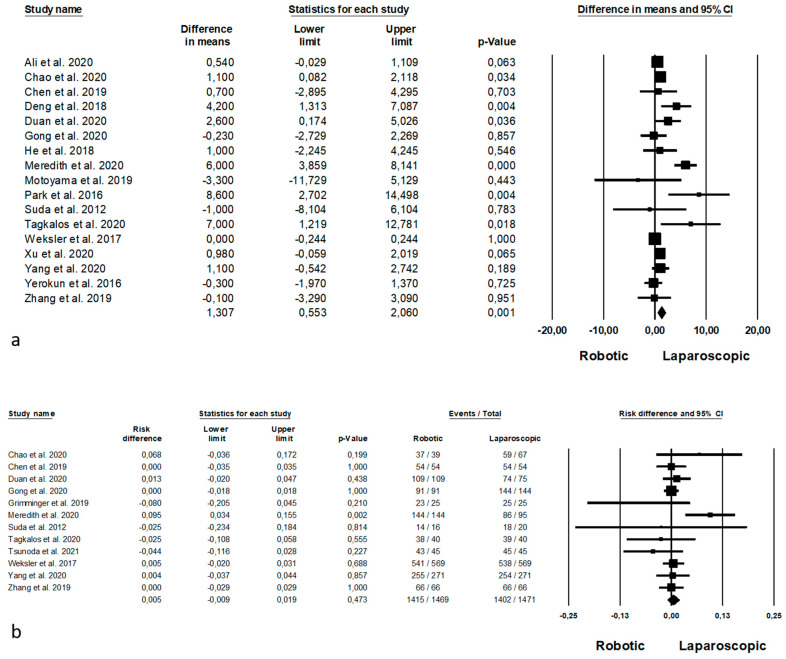
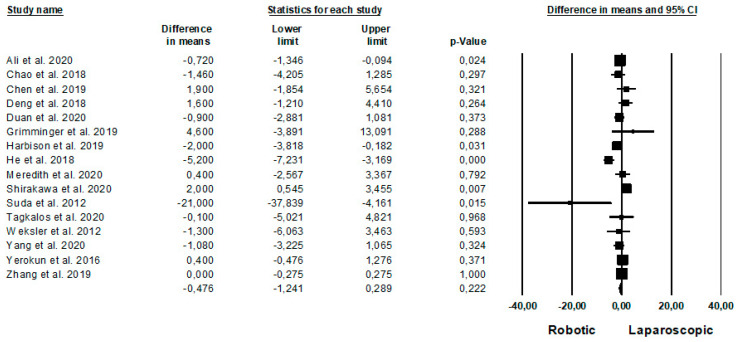
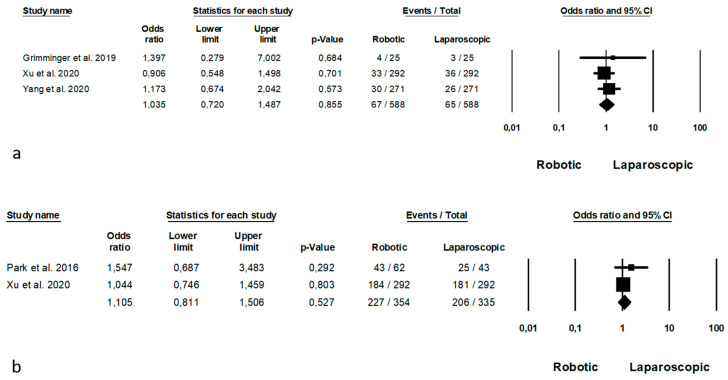
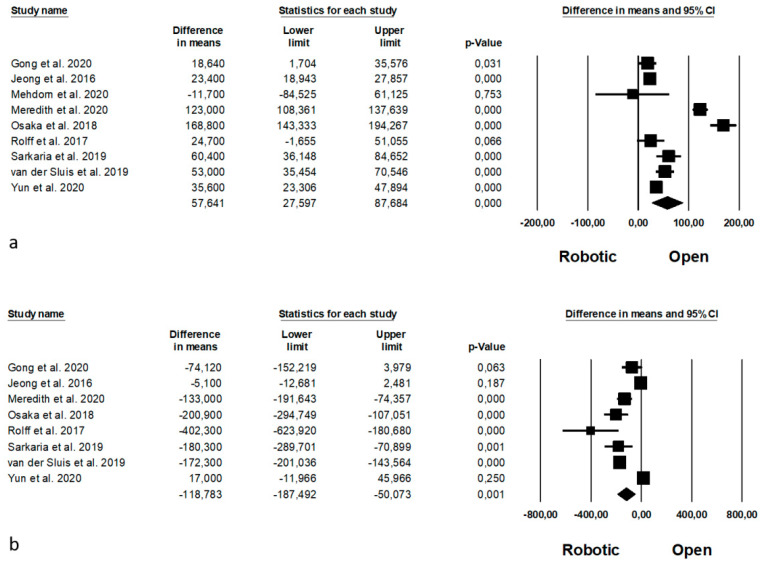
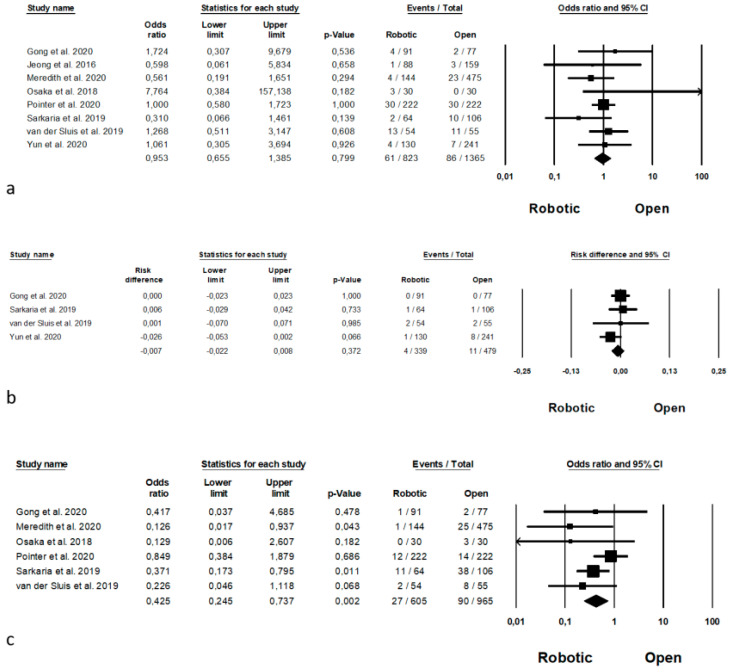
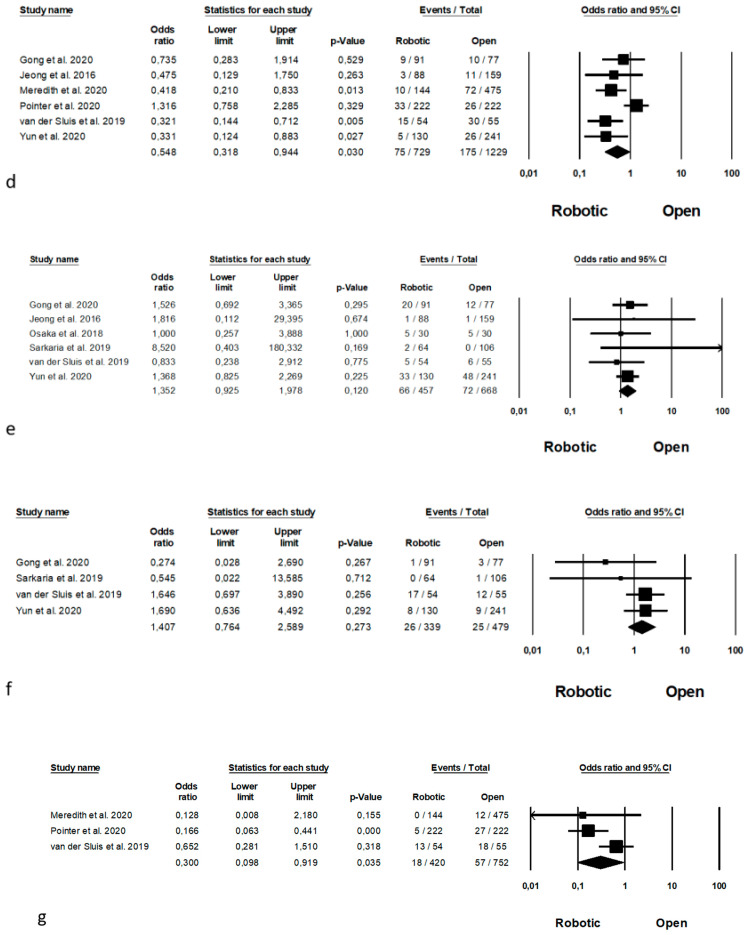
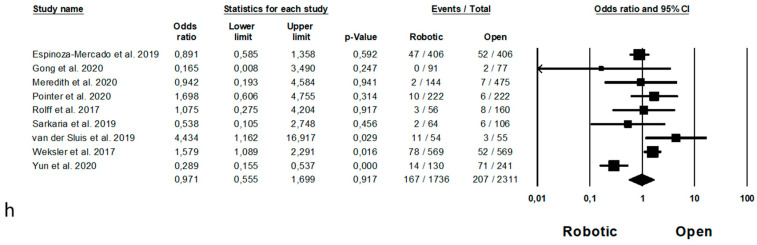
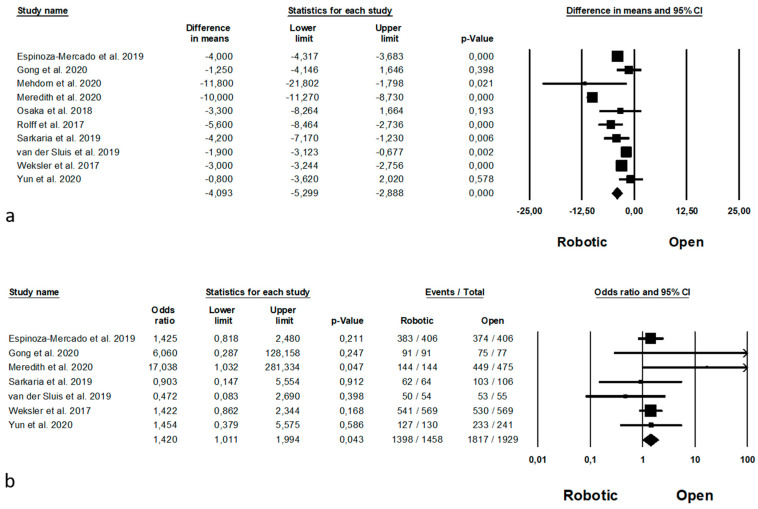
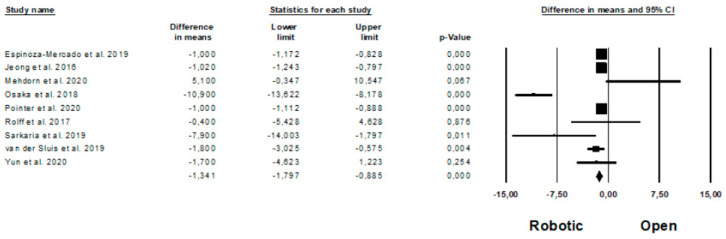
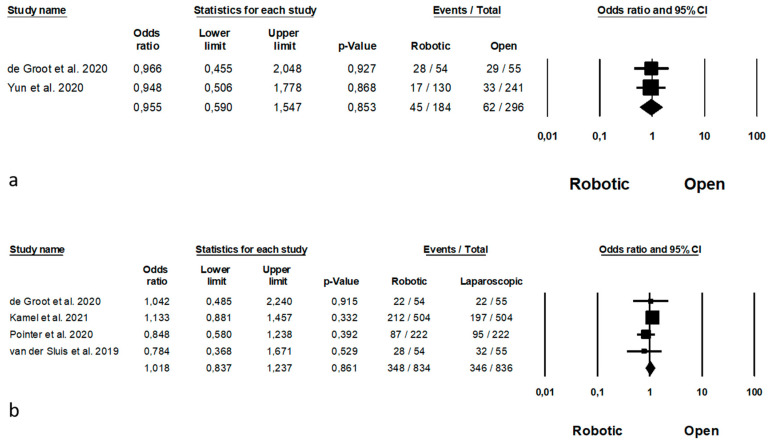
Background: Robot-Assisted Minimally Invasive Esophagectomy is demonstrated to be related with a facilitation in thoracoscopic procedure. To give an update on the state of art of robotic esophagectomy for cancr a systematic review with meta-analysis has been performed. Methods: a search of the studies comparing robotic and laparoscopic or open esophagectomy was performed trough the medical libraries, with the search string "robotic and (oesophagus OR esophagus OR esophagectomy OR oesophagectomy)". Outcomes were: postoperative complications rate (anastomotic leakage, bleeding, wound infection, pneumonia, recurrent laryngeal nerves paralysis, chylotorax, mortality), intraoperative outcomes (mean blood loss, operative time and conversion), oncologic outcomes (harvested nodes, R0 resection, recurrence) and recovery outcomes (length of hospital stay). Results: Robotic approach is superior to open surgery in terms of blood loss p = 0.001, wound infection rate, p = 0.002, pneumonia rate, p = 0.030 and mean number of harvested nodes, p < 0.0001 and R0 resection rate, p = 0.043. Similarly, robotic approach is superior to conventional laparoscopy in terms of mean number of harvested nodes, p = 0.001 pneumonia rate, p = 0.003. Conclusions: robotic surgery could be considered superior to both open surgery and conventional laparoscopy. These encouraging results should promote the diffusion of the robotic surgery, with the creation of randomized trials to overcome selection bias.
Keywords: esophageal cancer; esophagectomy; laparoscopic; open surgery; robotic.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
