

Endoscopic transsphenoidal surgery for resection of pituitary macroadenoma: A retrospective study
- PMID: 34358251
- PMCID: PMC8345891
- DOI: 10.1371/journal.pone.0255599
Endoscopic transsphenoidal surgery for resection of pituitary macroadenoma: A retrospective study
Abstract
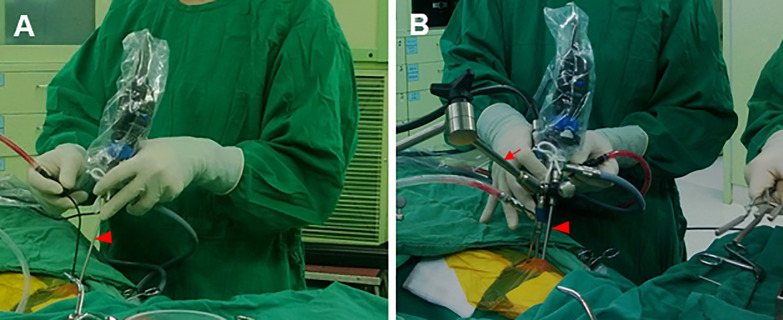
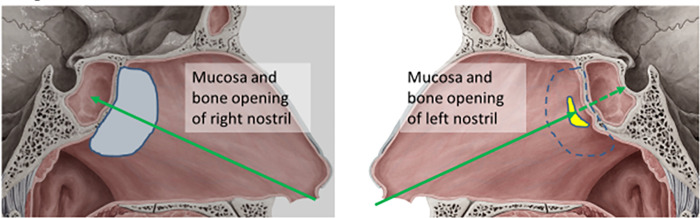
Background: The endoscopic transsphenoidal approach is an efficient minimally invasive procedure for removal of pituitary tumors that can be accomplished through a one-hand or two-hand approach. The one-hand procedure through one nostril is more intuitive for surgeons, but maneuvering the instruments can be restrictive. The two-hand procedure using a one-and-half nostril approach provides more precise manipulation. This study aimed to compare the surgical outcomes of one-hand/mono-nostril and two-hand/one-and-half nostril surgeries for resection of large pituitary tumors by a single neurosurgeon.
Materials and methods: The surgical data of 78 consecutive cases with pituitary macroadenoma (diameter >1 cm) were reviewed retrospectively. Altogether, 30 cases received one-hand/mono-nostril surgery, while 48 cases received two-hand/one-and-half nostril surgery. Postoperative outcomes of the two operations were compared.
Results: The operative time, hospital stay, residual rate of pituitary macroadenoma, visual field, surgical complications, and re-operative rates were slightly improved in the two-hand/one-and-half nostril surgery group compared with that in the one-hand/mono-nostril surgery group (all p>0.05). However, postoperative hypopituitarism was less frequent (1/48; 2.0%) with the two-hand/one-and-half nostril approach than with the mono-nostril approach (p = 0.004). Similar surgical outcomes were found in all patients with either small or large pituitary tumors, except that the difference in postoperative improvement in visual field change reached statistical significance (p = 0.044).
Conclusion: A single-surgeon endoscopic endonasal transsphenoidal surgery with two-hand/one-and-half nostril approach is an effective and safe procedure for removal of large pituitary tumors.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Kassam A, Snyderman CH, Carrau RL, Gardner P, Mintz A. Endoneurosurgical hemostasis techniques: lessons learned from 400 cases. Neurosurg Focus. 2005;19(1):E7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
