

Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2
- PMID: 34358472
- PMCID: PMC8443448
- DOI: 10.1016/S2352-4642(21)00198-X
Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2
Erratum in
-
Correction to Lancet Child Adolesc Health 2021; 5: 708-18.Lancet Child Adolesc Health. 2021 Oct;5(10):e43. doi: 10.1016/S2352-4642(21)00276-5. Epub 2021 Sep 1. Lancet Child Adolesc Health. 2021. PMID: 34478632 Free PMC article. No abstract available.
Abstract
Background: In children, SARS-CoV-2 infection is usually asymptomatic or causes a mild illness of short duration. Persistent illness has been reported; however, its prevalence and characteristics are unclear. We aimed to determine illness duration and characteristics in symptomatic UK school-aged children tested for SARS-CoV-2 using data from the COVID Symptom Study, one of the largest UK citizen participatory epidemiological studies to date.
Methods: In this prospective cohort study, data from UK school-aged children (age 5-17 years) were reported by an adult proxy. Participants were voluntary, and used a mobile application (app) launched jointly by Zoe Limited and King's College London. Illness duration and symptom prevalence, duration, and burden were analysed for children testing positive for SARS-CoV-2 for whom illness duration could be determined, and were assessed overall and for younger (age 5-11 years) and older (age 12-17 years) groups. Children with longer than 1 week between symptomatic reports on the app were excluded from analysis. Data from symptomatic children testing negative for SARS-CoV-2, matched 1:1 for age, gender, and week of testing, were also assessed.
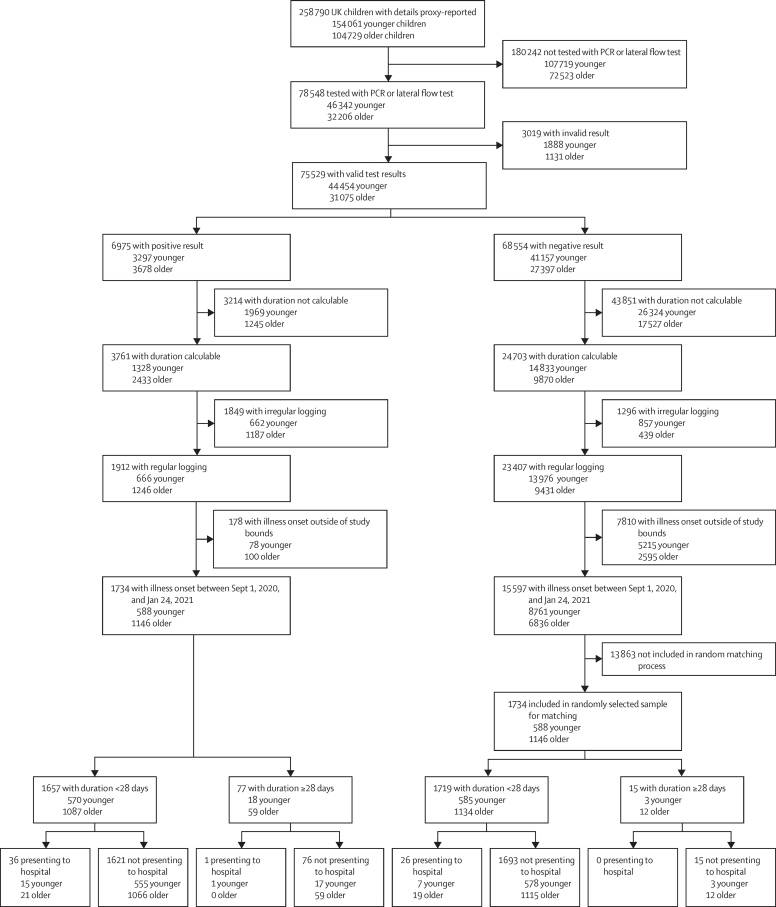
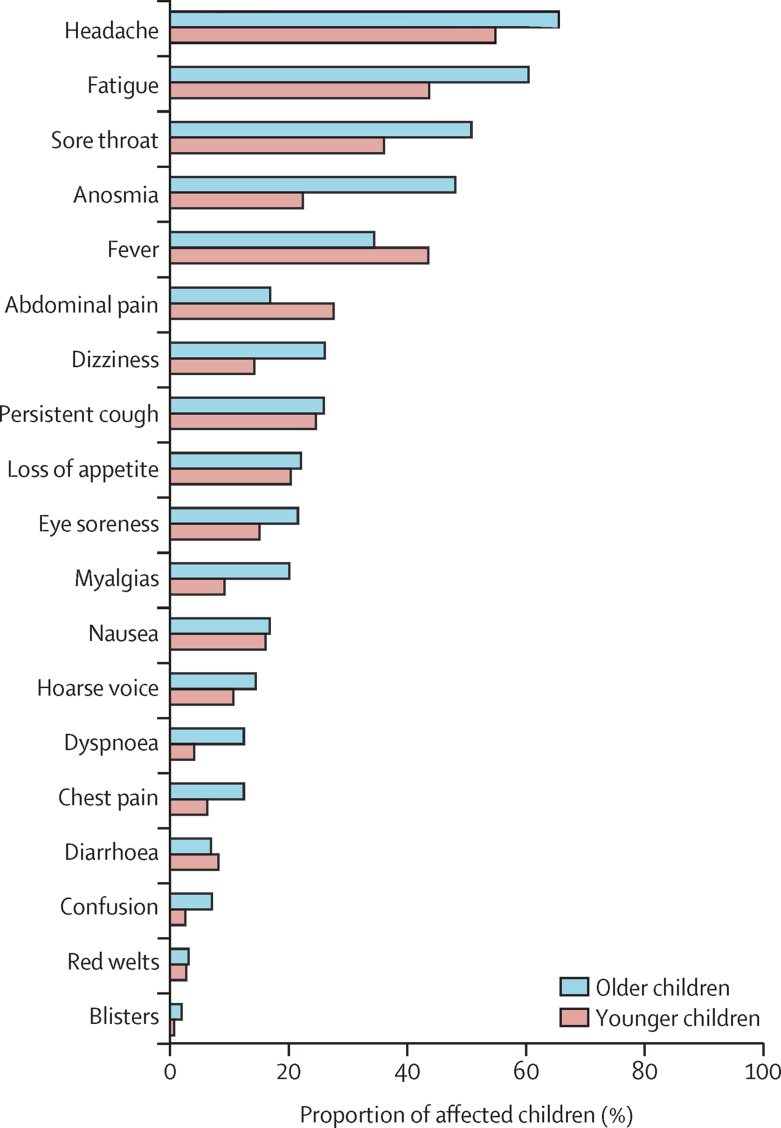
Findings: 258 790 children aged 5-17 years were reported by an adult proxy between March 24, 2020, and Feb 22, 2021, of whom 75 529 had valid test results for SARS-CoV-2. 1734 children (588 younger and 1146 older children) had a positive SARS-CoV-2 test result and calculable illness duration within the study timeframe (illness onset between Sept 1, 2020, and Jan 24, 2021). The most common symptoms were headache (1079 [62·2%] of 1734 children), and fatigue (954 [55·0%] of 1734 children). Median illness duration was 6 days (IQR 3-11) versus 3 days (2-7) in children testing negative, and was positively associated with age (Spearman's rank-order rs 0·19, p<0·0001). Median illness duration was longer for older children (7 days, IQR 3-12) than younger children (5 days, 2-9). 77 (4·4%) of 1734 children had illness duration of at least 28 days, more commonly in older than younger children (59 [5·1%] of 1146 older children vs 18 [3·1%] of 588 younger children; p=0·046). The commonest symptoms experienced by these children during the first 4 weeks of illness were fatigue (65 [84·4%] of 77), headache (60 [77·9%] of 77), and anosmia (60 [77·9%] of 77); however, after day 28 the symptom burden was low (median 2 symptoms, IQR 1-4) compared with the first week of illness (median 6 symptoms, 4-8). Only 25 (1·8%) of 1379 children experienced symptoms for at least 56 days. Few children (15 children, 0·9%) in the negatively tested cohort had symptoms for at least 28 days; however, these children experienced greater symptom burden throughout their illness (9 symptoms, IQR 7·7-11·0 vs 8, 6-9) and after day 28 (5 symptoms, IQR 1·5-6·5 vs 2, 1-4) than did children who tested positive for SARS-CoV-2.
Interpretation: Although COVID-19 in children is usually of short duration with low symptom burden, some children with COVID-19 experience prolonged illness duration. Reassuringly, symptom burden in these children did not increase with time, and most recovered by day 56. Some children who tested negative for SARS-CoV-2 also had persistent and burdensome illness. A holistic approach for all children with persistent illness during the pandemic is appropriate.
Funding: Zoe Limited, UK Government Department of Health and Social Care, Wellcome Trust, UK Engineering and Physical Sciences Research Council, UK Research and Innovation London Medical Imaging and Artificial Intelligence Centre for Value Based Healthcare, UK National Institute for Health Research, UK Medical Research Council, British Heart Foundation, and Alzheimer's Society.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests CH, SS, KR, and JCP are employees of Zoe Limited. TDS reports being a consultant for Zoe Limited, during the conduct of the study. All other authors declare no competing interests.
Figures


Comment in
-
Citizen science and biomedical research.Lancet Child Adolesc Health. 2021 Oct;5(10):682-683. doi: 10.1016/S2352-4642(21)00237-6. Epub 2021 Aug 3. Lancet Child Adolesc Health. 2021. PMID: 34358474 No abstract available.
-
Long COVID in children.Lancet Child Adolesc Health. 2022 Jan;6(1):e1. doi: 10.1016/S2352-4642(21)00338-2. Lancet Child Adolesc Health. 2022. PMID: 34921806 Free PMC article. No abstract available.
-
Long COVID in children.Lancet Child Adolesc Health. 2022 Jan;6(1):e2. doi: 10.1016/S2352-4642(21)00342-4. Lancet Child Adolesc Health. 2022. PMID: 34921807 Free PMC article. No abstract available.
-
Long COVID in children - Authors' reply.Lancet Child Adolesc Health. 2022 Jan;6(1):e3. doi: 10.1016/S2352-4642(21)00344-8. Lancet Child Adolesc Health. 2022. PMID: 34921808 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
