

Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management
- PMID: 34358489
- PMCID: PMC8564770
- DOI: 10.1053/j.gastro.2021.07.042
Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management
Abstract
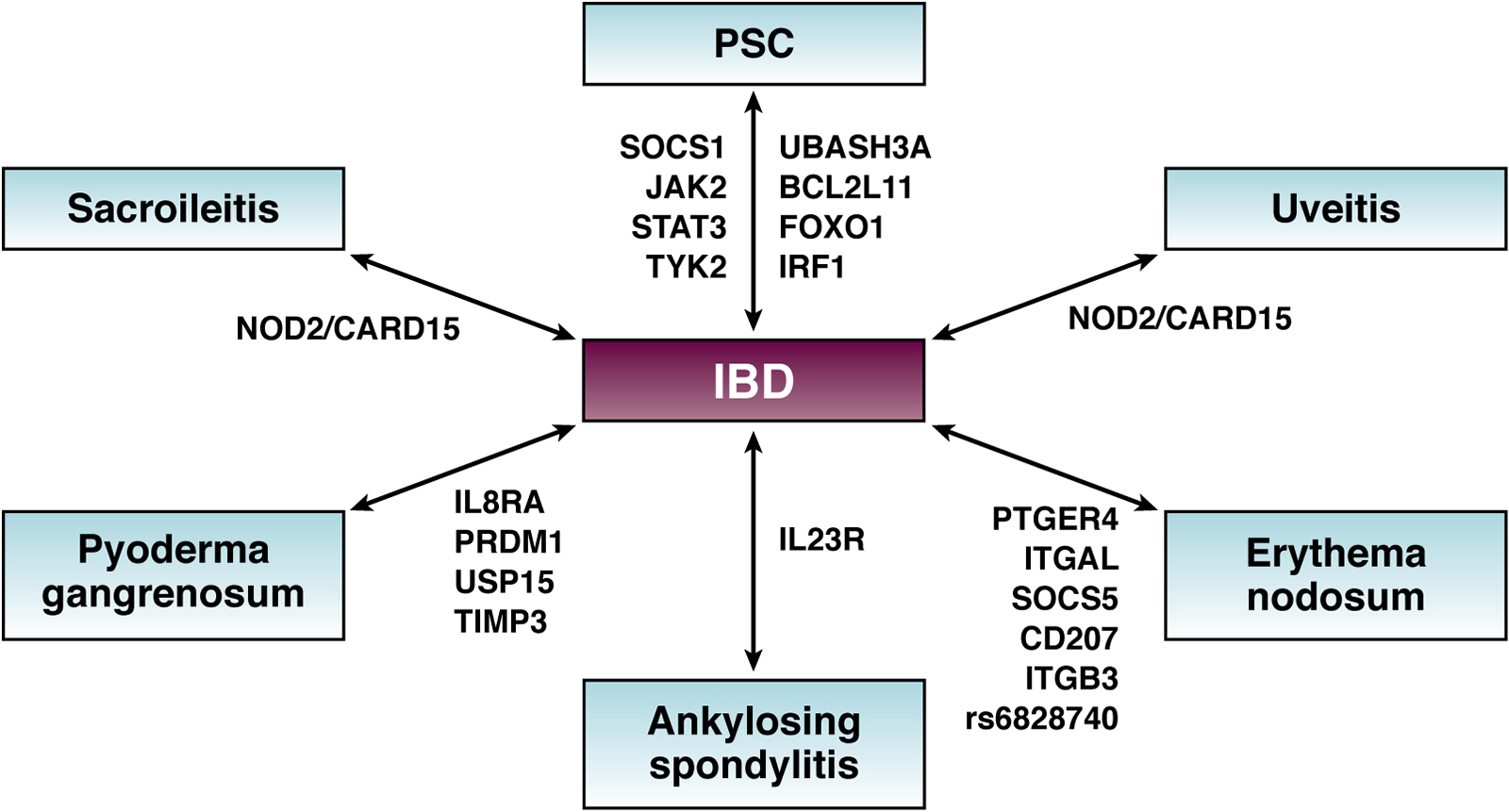
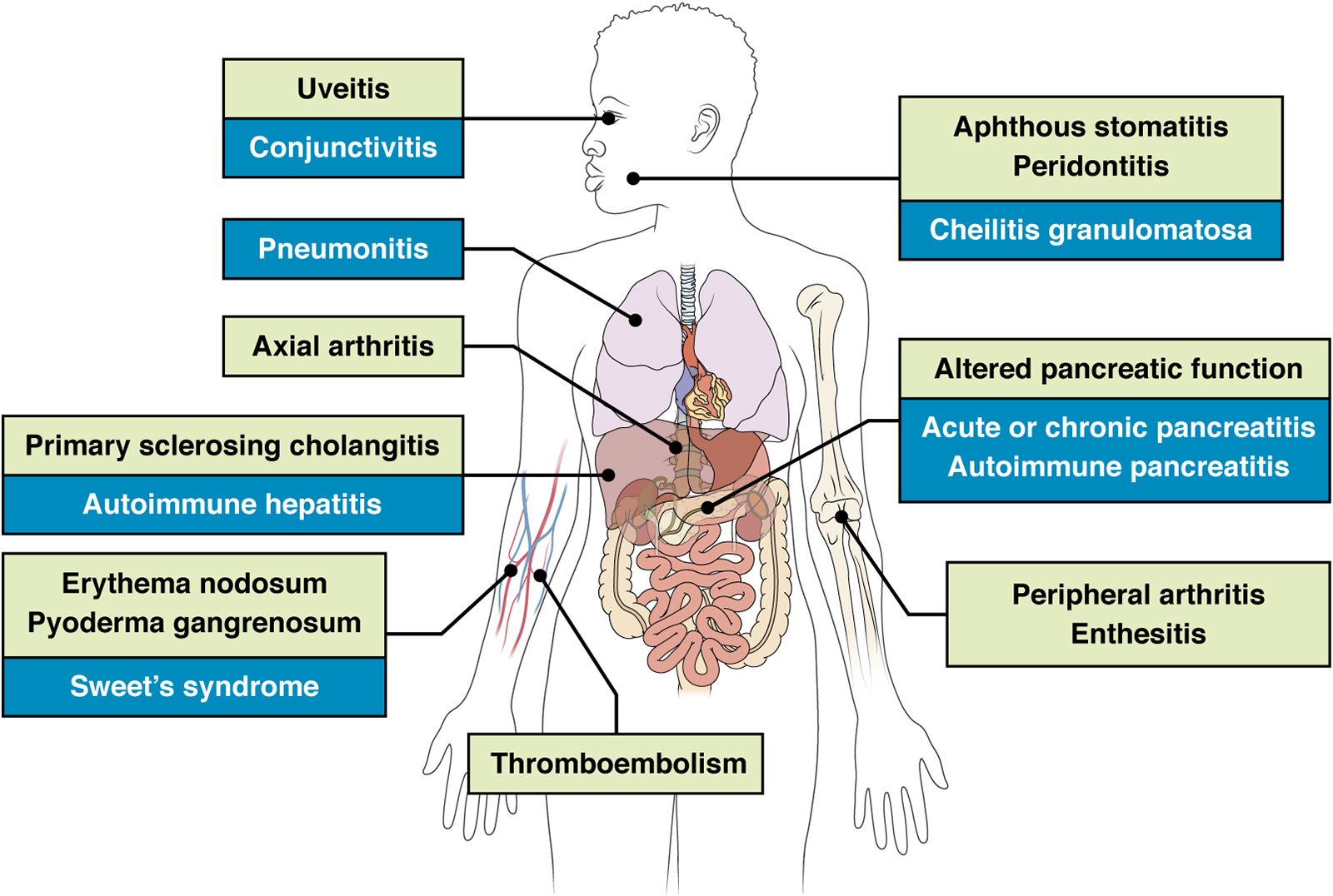
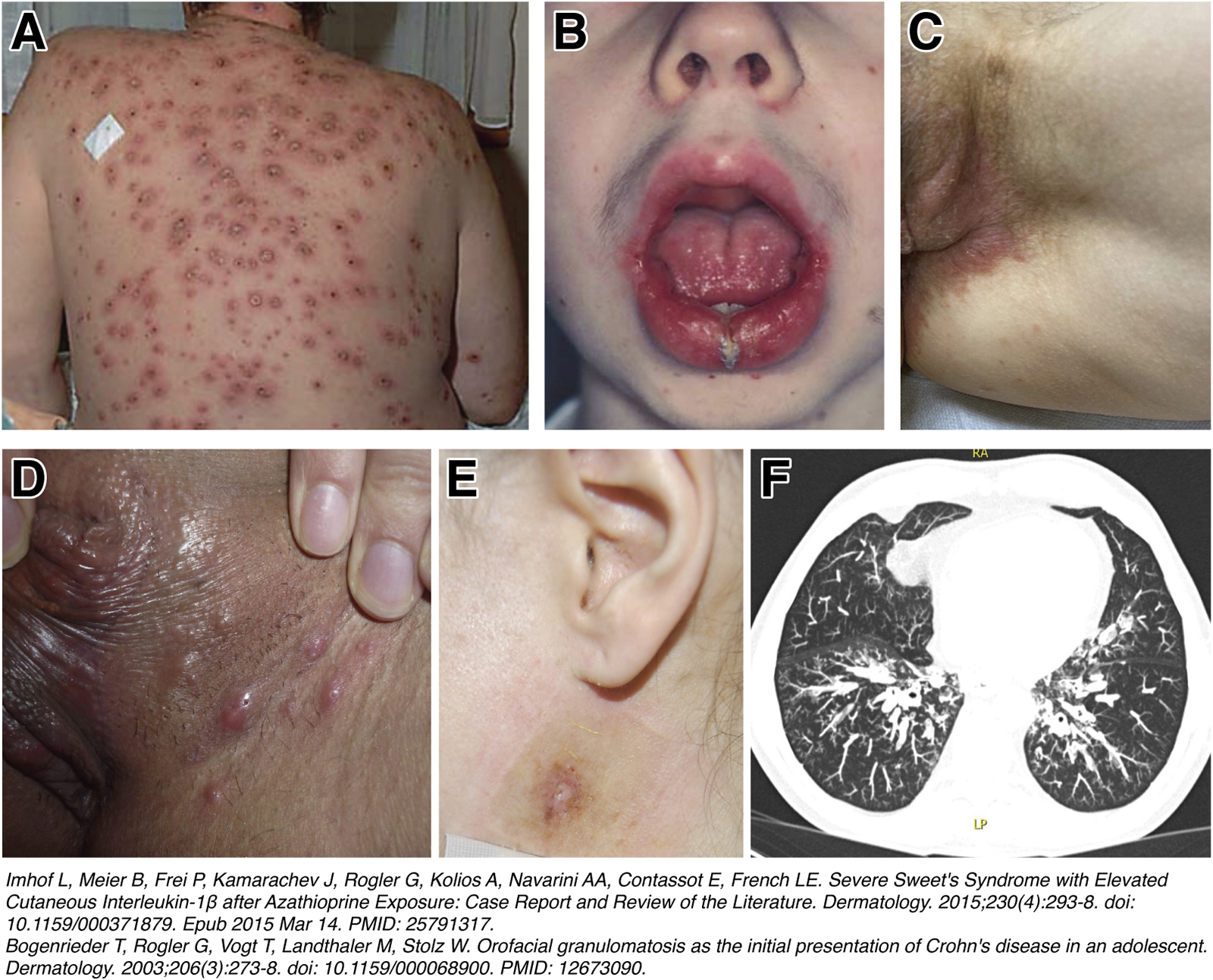
Inflammatory bowel diseases (IBDs) are systemic diseases that manifest not only in the gut and gastrointestinal tract, but also in the extraintestinal organs in many patients. The quality of life for patients with IBD can be substantially affected by these extraintestinal manifestations (EIMs). It is important to have knowledge of the prevalence, pathophysiology, and clinical presentation of EIMs in order to adapt therapeutic options to cover all aspects of IBD. EIMs can occur in up to 24% of patients with IBD before the onset of intestinal symptoms, and need to be recognized to initiate appropriate diagnostic procedures. EIMs most frequently affect joints, skin, or eyes, but can also affect other organs, such as the liver, lung, and pancreas. It is a frequent misconception that a successful therapy of the intestinal inflammation will be sufficient to treat EIMs satisfactorily in most patients with IBD. In general, peripheral arthritis, oral aphthous ulcers, episcleritis, or erythema nodosum can be associated with active intestinal inflammation and can improve on standard treatment of the intestinal inflammation. However, anterior uveitis, ankylosing spondylitis, and primary sclerosing cholangitis usually occur independent of disease flares. This review provides a comprehensive overview of epidemiology, pathophysiology, clinical presentation, and treatment of EIMs in IBD.
Keywords: Arthralgias; Arthritis; Crohn’s Disease; Erythema Nodosum; Extraintestinal Manifestations; Inflammatory Bowel Disease; Primary Sclerosing Cholangitis; Psoriasis; Pyoderma Gangrenosum; Spondyloarthropathy; Ulcerative Colitis; Uveitis.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Garber A, Regueiro M. Extraintestinal Manifestations of Inflammatory Bowel Disease: Epidemiology, Etiopathogenesis, and Management. Curr Gastroenterol Rep 2019;21:31. - PubMed
-
- Su CG, Judge TA, Lichtenstein GR. Extraintestinal manifestations of inflammatory bowel disease. Gastroenterol Clin North Am 2002;31:307–27. - PubMed
-
- Orchard T Extraintestinal complications of inflammatory bowel disease. Curr Gastroenterol Rep 2003;5:512–7. - PubMed
-
- Hedin CRH, Vavricka SR, Stagg AJ, et al. The Pathogenesis of Extraintestinal Manifestations: Implications for IBD Research, Diagnosis, and Therapy. J Crohns Colitis 2019;13:541–554. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
