

Post-Traumatic Intraparenchymal Renal Hemorrhages: Correlation between CT and DSA Vascular Findings for Superselective Embolization Procedures
- PMID: 34359339
- PMCID: PMC8305924
- DOI: 10.3390/diagnostics11071256
Post-Traumatic Intraparenchymal Renal Hemorrhages: Correlation between CT and DSA Vascular Findings for Superselective Embolization Procedures
Abstract
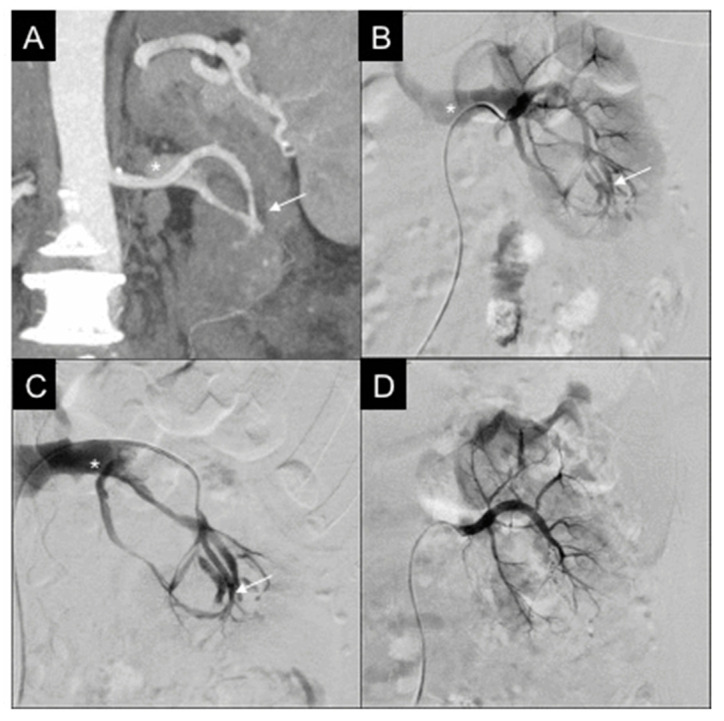
Background: This study aims to investigate the correlation between computed tomography (CT) and digital subtraction angiography (DSA) findings in patients affected by acute post-traumatic intraparenchymal renal hemorrhages and evaluate their conservative management with superselective embolization.
Methods: This retrospective multicenter analysis focuses on patients affected by renal bleedings detected by contrast-enhanced CT and treated with superselective endovascular embolization. CT findings were compared to DSA. Embolization procedural data were analyzed and renal function was evaluated before and after the intervention.
Results: Twenty-seven patients were retrospectively evaluated in one year. Compared to DSA, CT showed 96.3% diagnostic accuracy in terms of hemorrhage recognition; concerning the type of vascular lesion, there was discrepancy between CT and DSA in five cases. The technical success rate of embolization was 100%, while primary clinical success was 88.9%. The inferior parenchymal third was the most frequent site of renal injury. Microcoils were the most adopted embolics. Renal function did not change significantly before and after embolization.
Conclusions: CT has elevated diagnostic accuracy in detecting post-traumatic intraparenchymal renal hemorrhages; in a small percentage, the type of vascular lesion may differ from the findings observed at DSA. In this scenario, superselective embolization presents high clinical success with a low complication rate.
Keywords: computed tomography; intraparenchymal; renal hemorrhage; superselective embolization; trauma.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures


References
-
- Iacobellis F., Ierardi A.M., Mazzei M.A., Magenta Biasina A., Carrafiello G., Nicola R., Scaglione M. Dual-phase CT for the assessment of acute vascular injuries in high-energy blunt trauma: The imaging findings and management implications. Br. J. Radiol. 2016;89:20150952. doi: 10.1259/bjr.20150952. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
