

Hyperinsulinemia and Its Pivotal Role in Aging, Obesity, Type 2 Diabetes, Cardiovascular Disease and Cancer
- PMID: 34360563
- PMCID: PMC8345990
- DOI: 10.3390/ijms22157797
Hyperinsulinemia and Its Pivotal Role in Aging, Obesity, Type 2 Diabetes, Cardiovascular Disease and Cancer
Abstract
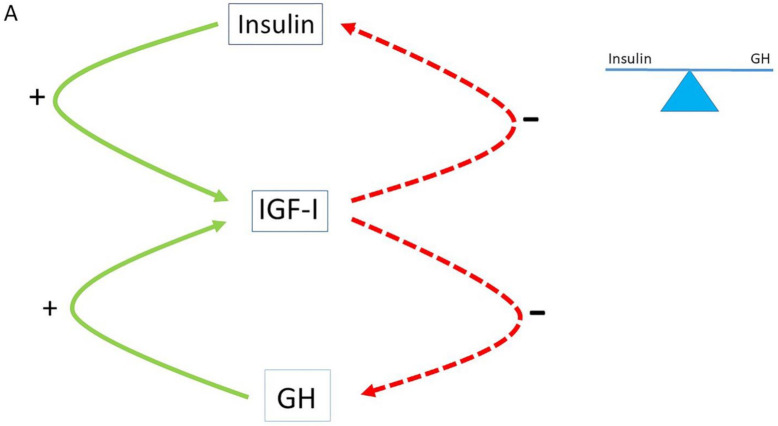
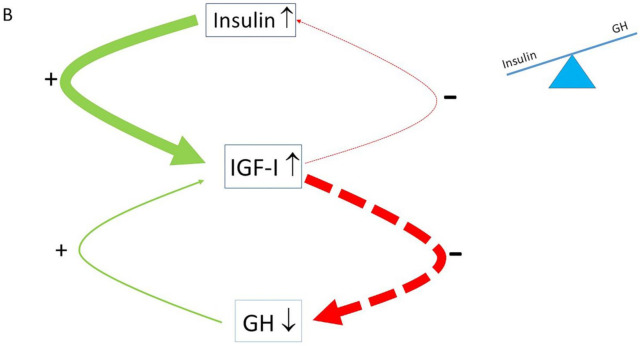
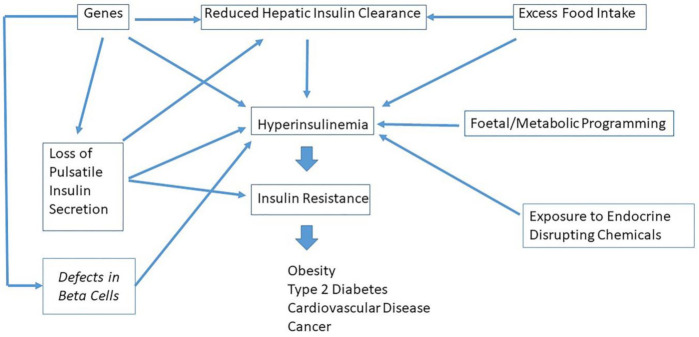
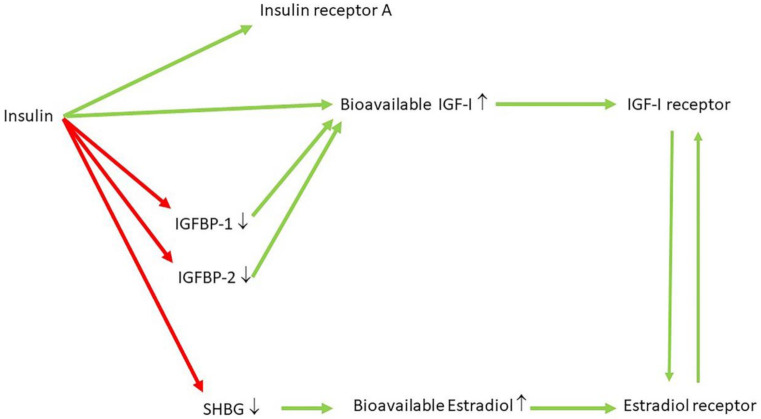
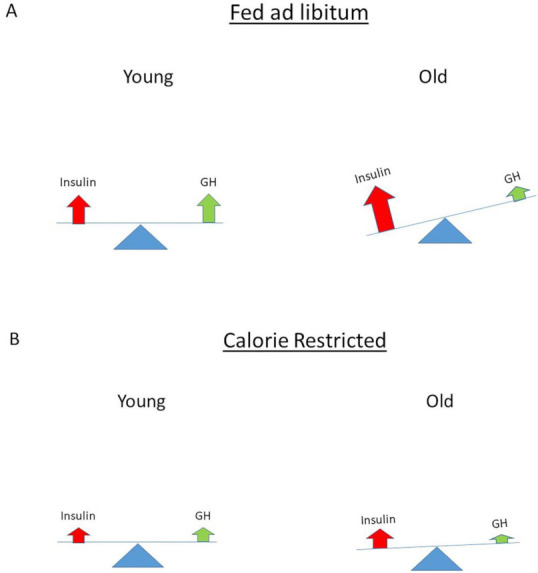
For many years, the dogma has been that insulin resistance precedes the development of hyperinsulinemia. However, recent data suggest a reverse order and place hyperinsulinemia mechanistically upstream of insulin resistance. Genetic background, consumption of the "modern" Western diet and over-nutrition may increase insulin secretion, decrease insulin pulses and/or reduce hepatic insulin clearance, thereby causing hyperinsulinemia. Hyperinsulinemia disturbs the balance of the insulin-GH-IGF axis and shifts the insulin : GH ratio towards insulin and away from GH. This insulin-GH shift promotes energy storage and lipid synthesis and hinders lipid breakdown, resulting in obesity due to higher fat accumulation and lower energy expenditure. Hyperinsulinemia is an important etiological factor in the development of metabolic syndrome, type 2 diabetes, cardiovascular disease, cancer and premature mortality. It has been further hypothesized that nutritionally driven insulin exposure controls the rate of mammalian aging. Interventions that normalize/reduce plasma insulin concentrations might play a key role in the prevention and treatment of age-related decline, obesity, type 2 diabetes, cardiovascular disease and cancer. Caloric restriction, increasing hepatic insulin clearance and maximizing insulin sensitivity are at present the three main strategies available for managing hyperinsulinemia. This may slow down age-related physiological decline and prevent age-related diseases. Drugs that reduce insulin (hyper) secretion, normalize pulsatile insulin secretion and/or increase hepatic insulin clearance may also have the potential to prevent or delay the progression of hyperinsulinemia-mediated diseases. Future research should focus on new strategies to minimize hyperinsulinemia at an early stage, aiming at successfully preventing and treating hyperinsulinemia-mediated diseases.
Keywords: cancer; cardiovascular disease; diabetes; growth hormone; hyperinsulinemia; insulin clearance; insulin resistance; insulin secretion; insulin-like growth factor-I; longevity; obesity.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
-
- Lakka H.M., Lakka T.A., Tuomilehto J., Sivenius J., Salonen J.T. Hyperinsulinemia and the risk of cardiovascular death and acute coronary and cerebrovascular events in men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Arch. Int. Med. 2000;160:1160–1168. doi: 10.1001/archinte.160.8.1160. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
