

Anti-Inflammatory Therapeutic Approaches to Prevent or Delay Post-Traumatic Osteoarthritis (PTOA) of the Knee Joint with a Focus on Sustained Delivery Approaches
- PMID: 34360771
- PMCID: PMC8347094
- DOI: 10.3390/ijms22158005
Anti-Inflammatory Therapeutic Approaches to Prevent or Delay Post-Traumatic Osteoarthritis (PTOA) of the Knee Joint with a Focus on Sustained Delivery Approaches
Abstract
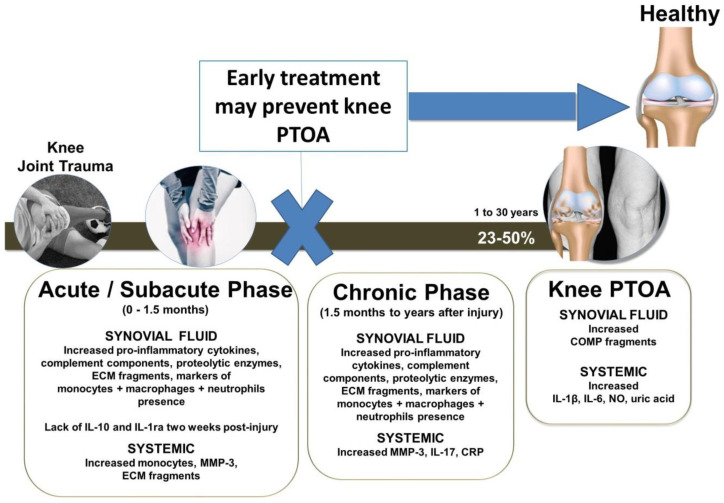
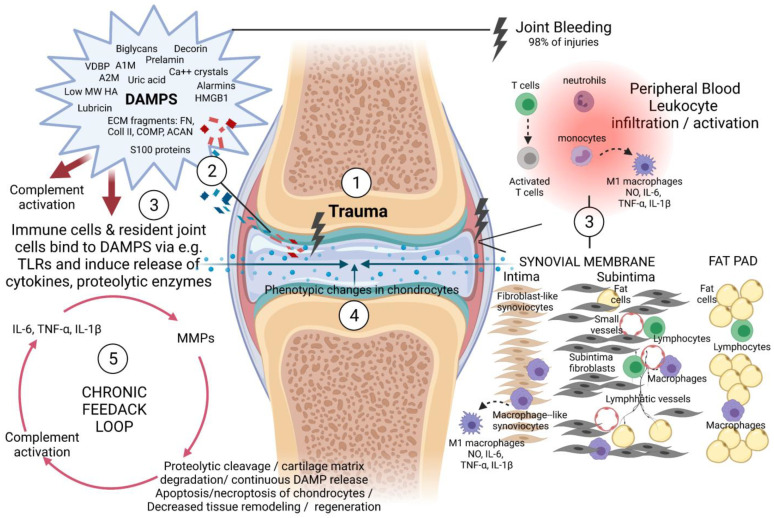
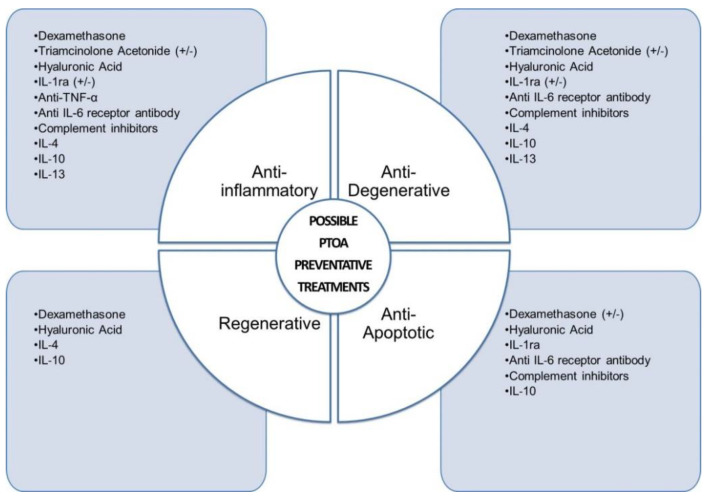
Inflammation plays a central role in the pathogenesis of knee PTOA after knee trauma. While a comprehensive therapy capable of preventing or delaying post-traumatic osteoarthritis (PTOA) progression after knee joint injury does not yet clinically exist, current literature suggests that certain aspects of early post-traumatic pathology of the knee joint may be prevented or delayed by anti-inflammatory therapeutic interventions. We discuss multifaceted therapeutic approaches that may be capable of effectively reducing the continuous cycle of inflammation and concomitant processes that lead to cartilage degradation as well as those that can simultaneously promote intrinsic repair processes. Within this context, we focus on early disease prevention, the optimal timeframe of treatment and possible long-lasting sustained delivery local modes of treatments that could prevent knee joint-associated PTOA symptoms. Specifically, we identify anti-inflammatory candidates that are not only anti-inflammatory but also anti-degenerative, anti-apoptotic and pro-regenerative.
Keywords: IL-1 receptor antagonist; IL-10; IL-13; IL-1β; IL-4; IL-6; TNF-α; anti-apoptotic; anti-inflammatory cytokines; antibody; articular cartilage; cartilage; cartilage repair; chondrocyte; clinical; complement inhibitors; complement system; degeneration; dexamethasone; drug delivery; early PTOA; early disease; fat pad; hyaluronic acid; immunomodulation; inflammation; knee joint; knee trauma; osteoarthritis; post-traumatic osteoarthritis; prevention; regeneration; synovium; tranexamic acid; triamcinolone acetonide.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Khella C.M., Asgarian R., Horvath J.M., Rolauffs B., Hart M.L. An evidence-based systematic review of human knee post-traumatic osteoarthritis (ptoa): Timeline of clinical presentation and disease markers, comparison of knee joint ptoa models and early disease implications. Int. J. Mol. Sci. 2021;22:1996. doi: 10.3390/ijms22041996. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
