

Multiomics Profiling Reveals Signatures of Dysmetabolism in Urban Populations in Central India
- PMID: 34361920
- PMCID: PMC8307859
- DOI: 10.3390/microorganisms9071485
Multiomics Profiling Reveals Signatures of Dysmetabolism in Urban Populations in Central India
Abstract
Background: Non-communicable diseases (NCDs) have become a major cause of morbidity and mortality in India. Perturbation of host-microbiome interactions may be a key mechanism by which lifestyle-related risk factors such as tobacco use, alcohol consumption, and physical inactivity may influence metabolic health. There is an urgent need to identify relevant dysmetabolic traits for predicting risk of metabolic disorders, such as diabetes, among susceptible Asian Indians where NCDs are a growing epidemic.
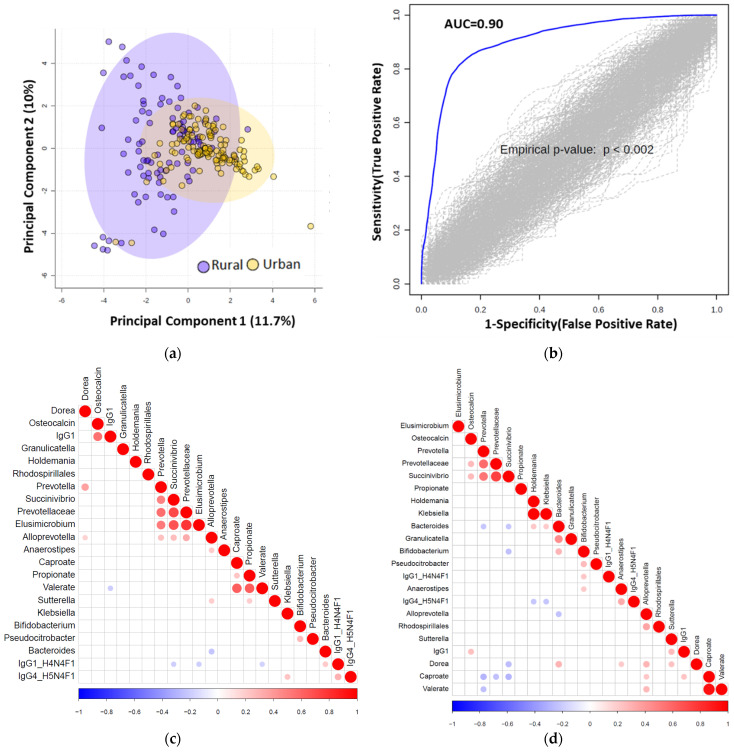
Methods: Here, we report the first in-depth phenotypic study in which we prospectively enrolled 218 adults from urban and rural areas of Central India and used multiomic profiling to identify relationships between microbial taxa and circulating biomarkers of cardiometabolic risk. Assays included fecal microbiota analysis by 16S ribosomal RNA gene amplicon sequencing, quantification of serum short chain fatty acids by gas chromatography-mass spectrometry, and multiplex assaying of serum diabetic proteins, cytokines, chemokines, and multi-isotype antibodies. Sera was also analysed for N-glycans and immunoglobulin G Fc N-glycopeptides.
Results: Multiple hallmarks of dysmetabolism were identified in urbanites and young overweight adults, the majority of whom did not have a known diagnosis of diabetes. Association analyses revealed several host-microbe and metabolic associations.
Conclusions: Host-microbe and metabolic interactions are differentially shaped by body weight and geographic status in Central Indians. Further exploration of these links may help create a molecular-level map for estimating risk of developing metabolic disorders and designing early interventions.
Keywords: diabetes mellitus; dysmetabolism; geography; glycome; host–microbe interactions; multiomics.
Conflict of interest statement
T.M. has received consultancy fees from Takeda. B.H.M. has received consultancy fees from Finch Therapeutics Group. J.R.M. has received consultancy fees from Cultech Ltd., and Enterobiotix Ltd. G.L. is founder and CEO of Genos, a private research organization that specializes in high-throughput glycomic analysis and has several patents in this field. M.P-B., F.K. and F.V. are employees of Genos. The remaining authors declare no competing interests.
Figures




References
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
