

Pulmonary Complications in Hematopoietic Stem Cell Transplant Recipients-A Clinician Primer
- PMID: 34362012
- PMCID: PMC8348211
- DOI: 10.3390/jcm10153227
Pulmonary Complications in Hematopoietic Stem Cell Transplant Recipients-A Clinician Primer
Abstract
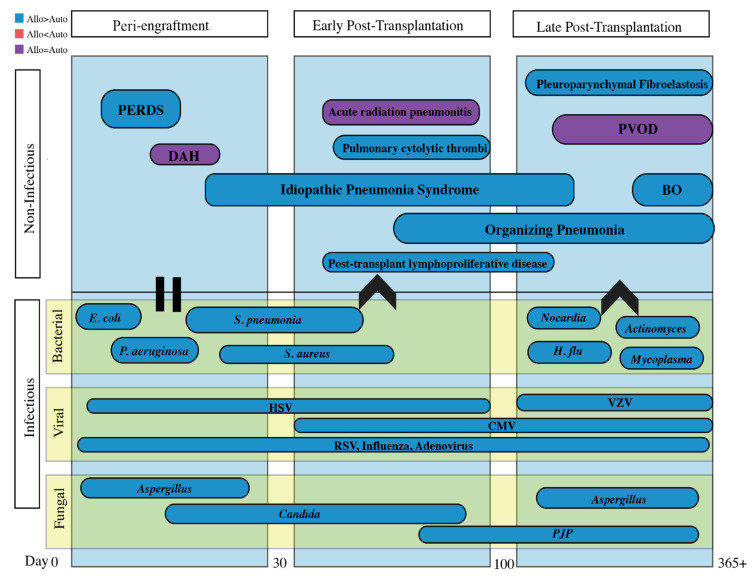
Hematopoietic stem cell transplants (HSCT) are becoming more widespread as a result of optimization of conditioning regimens and prevention of short-term complications with prophylactic antibiotics and antifungals. However, pulmonary complications post-HSCT remain a leading cause of morbidity and mortality and are a challenge to clinicians in both diagnosis and treatment. This comprehensive review provides a primer for non-pulmonary healthcare providers, synthesizing the current evidence behind common infectious and non-infectious post-transplant pulmonary complications based on time (peri-engraftment, early post-transplantation, and late post-transplantation). Utilizing the combination of timing of presentation, clinical symptoms, histopathology, and radiographic findings should increase rates of early diagnosis, treatment, and prognostication of these severe illness states.
Keywords: DAH; IPS; PERDS; bronchiolitis obliterans syndrome; post-HSCT.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Cordonnier C., Bernaudin J.F., Bierling P., Huet Y., Vernant J.P. Pulmonary complications occurring after allogeneic bone marrow transplantation. A study of 130 consecutive transplanted patients. Cancer. 1986;58:1047–1054. doi: 10.1002/1097-0142(19860901)58:5<1047::AID-CNCR2820580512>3.0.CO;2-Y. - DOI - PubMed
-
- Forman S.J., Negrin R.S., Antin J.H., Appelbaum F.R. Thomas’ Hematopoietic Cell Transplantation. Wiley Blackwell; Hoboken, NJ, USA: 2016.
