

Dynamic Left Intraventricular Obstruction Phenotype in Takotsubo Syndrome
- PMID: 34362020
- PMCID: PMC8347696
- DOI: 10.3390/jcm10153235
Dynamic Left Intraventricular Obstruction Phenotype in Takotsubo Syndrome
Abstract
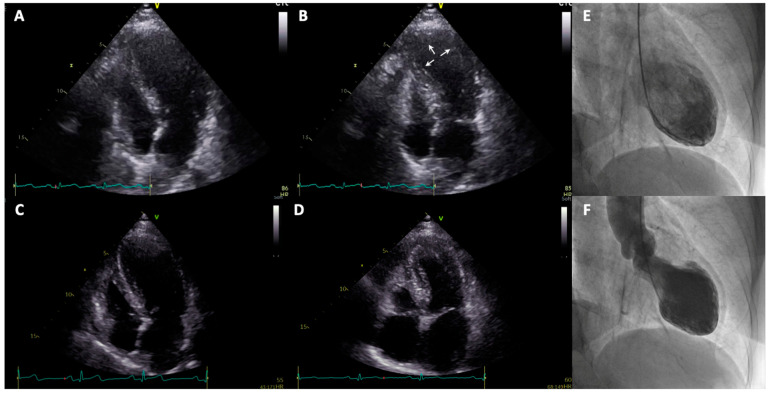
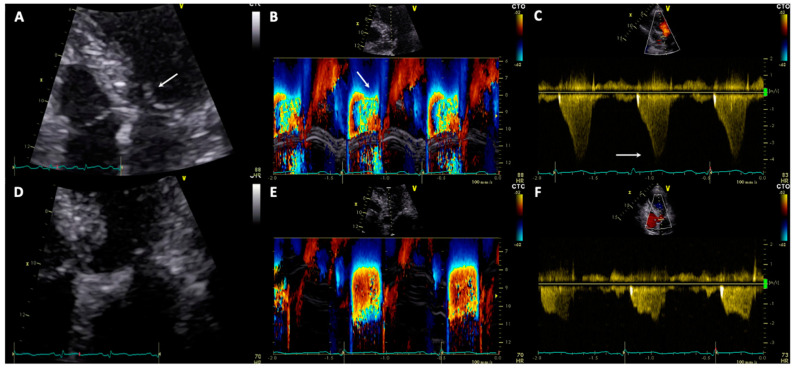
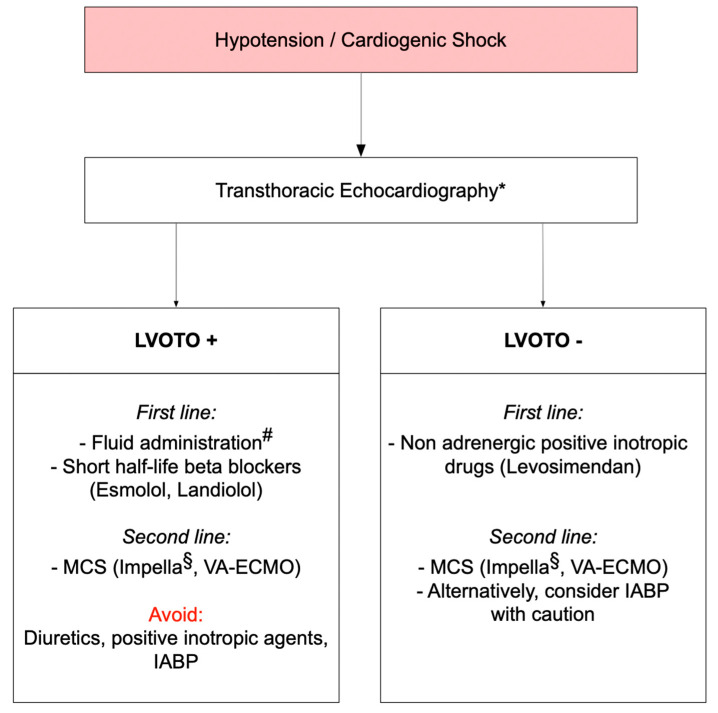
Takotsubo syndrome (TTS) is characterized by acute, generally transient left ventricular (LV) dysfunction. Although TTS has been long regarded as a benign condition, recent evidence showed that rate of acute complications and in-hospital mortality is comparable to that of patients with acute coronary syndrome. In particular, the prevalence of cardiogenic shock ranges between 6% and 20%. In this setting, detection of mechanisms leading to cardiogenic shock can be challenging. Besides a severely impaired systolic function, onset of LV outflow tract obstruction (LVOTO) together with mitral regurgitation related to systolic anterior motion of mitral valve leaflets can lead to hemodynamic instability. Early identification of LVOTO with echocardiography is crucial and has important implications on selection of the appropriate therapy. Application of short-acting b1-selective betablockers and prudent administration of fluids might help to resolve LVOTO. Conversely, inotrope agents may increase basal hypercontractility and worsen the intraventricular pressure gradient. To date, outcomes and management of patients with TTS complicated by LVOTO as yet has not been comprehensively investigated.
Keywords: Takotsubo syndrome; cardiogenic shock; echocardiography; heart failure; left ventricular outflow tract obstruction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Takotsubo syndrome complicated by cardiogenic shock due to left ventricular outflow tract obstruction, acute mitral regurgitation, and atrial fibrillation: a case report.Eur Heart J Case Rep. 2024 Jul 31;8(8):ytae367. doi: 10.1093/ehjcr/ytae367. eCollection 2024 Aug. Eur Heart J Case Rep. 2024. PMID: 39139854 Free PMC article.
-
Impella in Takotsubo syndrome complicated by left ventricular outflow tract obstruction and severe mitral regurgitation.ESC Heart Fail. 2020 Feb;7(1):306-310. doi: 10.1002/ehf2.12546. Epub 2020 Jan 3. ESC Heart Fail. 2020. PMID: 31898420 Free PMC article.
-
Left ventricular outflow tract obstruction in Takotsubo syndrome with cardiogenic shock: prognosis and treatment.Heart. 2024 Nov 19;110(23):1381-1388. doi: 10.1136/heartjnl-2024-324205. Heart. 2024. PMID: 39209437
-
Cardiogenic shock in takotsubo syndrome: etiology and treatment.Cardiovasc Interv Ther. 2024 Oct;39(4):421-427. doi: 10.1007/s12928-024-01031-3. Epub 2024 Jul 22. Cardiovasc Interv Ther. 2024. PMID: 39039401 Free PMC article. Review.
-
Management of Takotsubo Syndrome: A Comprehensive Review.Cureus. 2020 Jan 3;12(1):e6556. doi: 10.7759/cureus.6556. Cureus. 2020. PMID: 32042529 Free PMC article. Review.
Cited by
-
Takotsubo Cardiomyopathy: Patients Characteristics, Mortality, and Clinical Significance of Left Ventricular Outflow Tract Gradient, Retrospective Study.Cardiol Res Pract. 2024 Jul 9;2024:5549795. doi: 10.1155/2024/5549795. eCollection 2024. Cardiol Res Pract. 2024. PMID: 39015408 Free PMC article.
-
Obesity Paradox in Takotsubo Syndrome Among Septic ICU Patients: A Retrospective Cohort Study.J Clin Med. 2025 Apr 11;14(8):2635. doi: 10.3390/jcm14082635. J Clin Med. 2025. PMID: 40283464 Free PMC article.
-
Perioperative management of Takotsubo cardiomyopathy: an overview.J Anesth Analg Crit Care. 2024 Jul 15;4(1):45. doi: 10.1186/s44158-024-00178-y. J Anesth Analg Crit Care. 2024. PMID: 39010210 Free PMC article. Review.
-
Takotsubo Syndrome: From Bench to Bedside and Bedside to Bench.J Clin Med. 2022 Aug 11;11(16):4704. doi: 10.3390/jcm11164704. J Clin Med. 2022. PMID: 36012945 Free PMC article.
-
Acute Coronary Syndrome in Patients with SARS-CoV-2 Infection: Pathophysiology and Translational Perspectives.Transl Med UniSa. 2022 Aug 29;24(2):1-11. doi: 10.37825/2239-9754.1034. eCollection 2022. Transl Med UniSa. 2022. PMID: 36447945 Free PMC article.
References
-
- Kurisu S., Sato H., Kawagoe T., Ishihara M., Shimatani Y., Nishioka K., Kono Y., Umemura T., Nakamura S. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm. In: Kodama K., Haze K., Hori M., editors. Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure. Kagakuhyoronsha Publishing Co.; Tokyo, Japan: 1990. pp. 56–64. (In Japanese)
-
- Kurisu S., Inoue I., Kawagoe T., Ishihara M., Shimatani Y., Nakamura S., Yoshida M., Mitsuba N., Hata T., Sato H. Time course of electrocardiographic changes in patients with tako-tsubo syndrome: Comparison with acute myocardial infarction with minimal enzymatic release. Circ. J. 2004;68:77–81. doi: 10.1253/circj.68.77. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
