

Understanding Chronic Venous Disease: A Critical Overview of Its Pathophysiology and Medical Management
- PMID: 34362022
- PMCID: PMC8348673
- DOI: 10.3390/jcm10153239
Understanding Chronic Venous Disease: A Critical Overview of Its Pathophysiology and Medical Management
Abstract
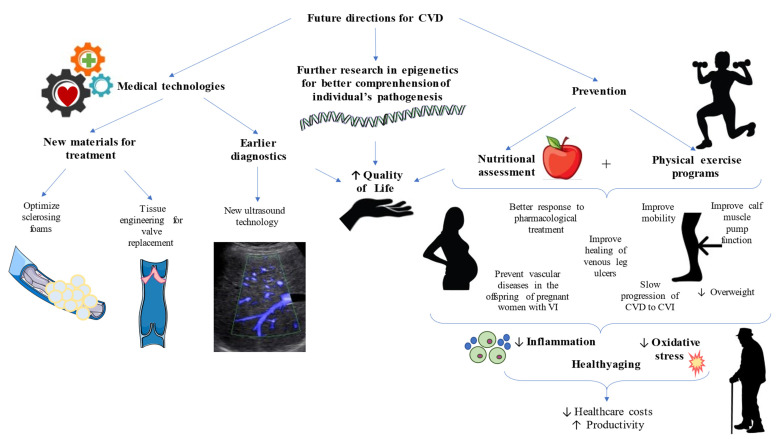
Chronic venous disease (CVD) is a multifactorial condition affecting an important percentage of the global population. It ranges from mild clinical signs, such as telangiectasias or reticular veins, to severe manifestations, such as venous ulcerations. However, varicose veins (VVs) are the most common manifestation of CVD. The explicit mechanisms of the disease are not well-understood. It seems that genetics and a plethora of environmental agents play an important role in the development and progression of CVD. The exposure to these factors leads to altered hemodynamics of the venous system, described as ambulatory venous hypertension, therefore promoting microcirculatory changes, inflammatory responses, hypoxia, venous wall remodeling, and epigenetic variations, even with important systemic implications. Thus, a proper clinical management of patients with CVD is essential to prevent potential harms of the disease, which also entails a significant loss of the quality of life in these individuals. Hence, the aim of the present review is to collect the current knowledge of CVD, including its epidemiology, etiology, and risk factors, but emphasizing the pathophysiology and medical care of these patients, including clinical manifestations, diagnosis, and treatments. Furthermore, future directions will also be covered in this work in order to provide potential fields to explore in the context of CVD.
Keywords: chronic venous disease (CVD); varicose veins; vascular therapies; venous hypertension; venous pathophysiology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
