

Neo-CheckRay: radiation therapy and adenosine pathway blockade to increase benefit of immuno-chemotherapy in early stage luminal B breast cancer, a randomized phase II trial
- PMID: 34362344
- PMCID: PMC8343924
- DOI: 10.1186/s12885-021-08601-1
Neo-CheckRay: radiation therapy and adenosine pathway blockade to increase benefit of immuno-chemotherapy in early stage luminal B breast cancer, a randomized phase II trial
Abstract
Background: Residual breast cancer after neo-adjuvant chemotherapy (NACT) predicts disease outcome and is a surrogate for survival in aggressive breast cancer (BC) subtypes. Pathological complete response (pCR) rate, however, is lower for luminal B BC in comparison to the triple negative (TNBC) and HER2+ subtypes. The addition of immune checkpoint blockade (ICB) to NACT has the potential to increase pCR rate but is hampered by the lower immunogenicity of luminal B BC. Novel strategies are needed to stimulate the immune response and increase the response rate to ICB in luminal B BC.
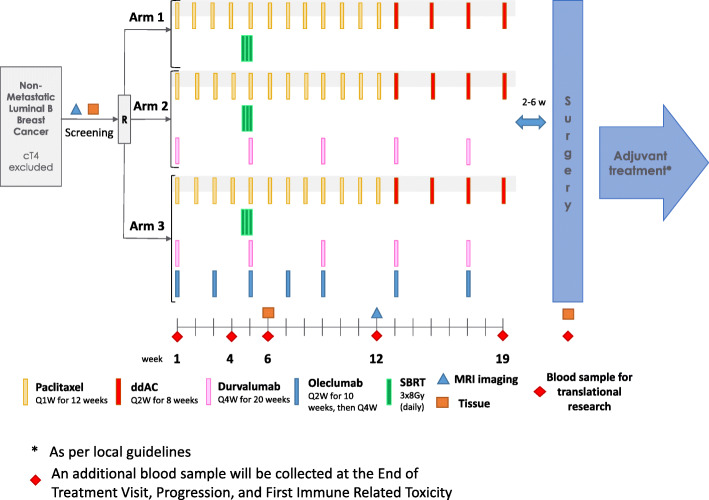
Methods: The Neo-CheckRay trial is a randomized phase II trial investigating the impact of stereotactic body radiation therapy (SBRT) to the primary breast tumor in combination with an anti-CD73 (oleclumab) to increase response to anti PD-L1 (durvalumab) and NACT. The trial is designed as a three-arm study: NACT + SBRT +/- durvalumab +/- oleclumab. The result at surgery will be evaluated using the residual cancer burden (RCB) index as the primary endpoint. Six patients will be included in a safety run-in, followed by a randomized phase II trial that will include 136 evaluable patients in 3 arms. Inclusion is limited to luminal B breast cancers that are MammaPrint genomic high risk.
Discussion: combination of ICB with chemotherapy in luminal B BC might benefit from immune priming agents to increase the response rate. As none have been identified so far, this phase II trial will evaluate SBRT and oleclumab as potential immune priming candidates.
Trial registration: trial registered on ClinicalTrials.gov ( NCT03875573 ) on March 14th, 2019.
Keywords: Anti-CD73; Anti-PD-L1; Early luminal B breast cancer; Neo-adjuvant chemotherapy; Priming; Stereotactic body radiation therapy.
© 2021. The Author(s).
Conflict of interest statement
ADC: institutional research grant from AstraZeneca. LB: institutional research grant from AstraZeneca; speaker honoraria from BMS; travel grant from Roche. PP: part-time medical advisor for Sordina IORT Technologies s.p.a., since 1 April 2020, not related to this work. DVG: Advisory board/Honoraria received: Sanofi, Accuray, Merck-Pfizer, Takeda and Novartis. RS: non-financial support from Merck, non-financial support from BMS, other from Puma Biotechnology, other from Roche, other from Roche, other from Merck. DE: Research Funding (ESMO Fellowship): Novartis. Speaker fee: Janssen. MP: Board Member (Scientific Board): Oncolytics; Consultant (honoraria): AstraZeneca, Camel-IDS, Crescendo Biologics, Debiopharm, G1 Therapeutics, Genentech, Huya, Immunomedics, Lilly, Menarini, MSD, Novartis, Odonate, Periphagen, Pfizer, Roche, Seattle Genetics. Research grants to my Institute: AstraZeneca, Lilly, MSD, Novartis, Pfizer, Radius, Roche-Genetech, Servier, Synthon. No stock ownership. ER: no disclosures relevant to this project. MI: Consultant or advisory role (honoraria): Celgene, Novartis, Pfizer, Seattle Genetics, Tesaro. Research grants to my Institute: Roche, Menarini Silicon Biosystems, Janssen Diagnostics, Pfizer. No stock ownership. Travel grants: Pfizer, Amgen. All other authors: no competing interests disclosed.
Figures
References
-
- Sorlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, Hastie T, Eisen MB, van de Rijn M, Jeffrey SS, Thorsen T, Quist H, Matese JC, Brown PO, Botstein D, Lonning PE, Borresen-Dale AL. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci U S A. 2001;98(19):10869–10874. doi: 10.1073/pnas.191367098s. - DOI - PMC - PubMed
-
- Bonnefoi H, Litière S, Piccart M, MacGrogan G, Fumoleau P, Brain E, et al. Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: a landmark and two-step approach analyses from the EORTC 10994/BIG 1-00 phase III trial. Ann Oncol. 014;25(6):1128–36. 10.1093/annonc/mdu118. - PMC - PubMed
-
- Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, Liu MC, Lluch A, Staroslawska E, de la Haba-Rodriguez J, Im SA, Pedrini JL, Poirier B, Morandi P, Semiglazov V, Srimuninnimit V, Bianchi G, Szado T, Ratnayake J, Ross G, Valagussa P. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13(1):25–32. doi: 10.1016/S1470-2045(11)70336-9. - DOI - PubMed
-
- Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L, Valagussa P, Swain SM, Prowell T, Loibl S, Wickerham DL, Bogaerts J, Baselga J, Perou C, Blumenthal G, Blohmer J, Mamounas EP, Bergh J, Semiglazov V, Justice R, Eidtmann H, Paik S, Piccart M, Sridhara R, Fasching PA, Slaets L, Tang S, Gerber B, Geyer CE, Jr, Pazdur R, Ditsch N, Rastogi P, Eiermann W, von Minckwitz G. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. doi: 10.1016/S0140-6736(13)62422-8. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
