

Experience with cultured thymus tissue in 105 children
- PMID: 34362576
- PMCID: PMC8810898
- DOI: 10.1016/j.jaci.2021.06.028
Experience with cultured thymus tissue in 105 children
Abstract
Background: Currently, there are no approved therapies to treat congenital athymia, a condition of immune deficiency resulting in high early mortality due to infection and immune dysregulation. Multiple syndromic conditions, such as complete DiGeorge syndrome, 22q11.2 deletion syndrome, CHARGE (coloboma, heart defects, choanal atresia, growth or mental retardation, genital hypoplasia, and ear anomalies and/or deafness) syndrome, diabetic embryopathy, other genetic variants, and FOXN1 deficiency, are associated with congenital athymia.
Objective: Our aims were to study 105 patients treated with cultured thymus tissue (CTT), and in this report, to focus on the outcomes of 95 patients with treatment-naive congenital athymia.
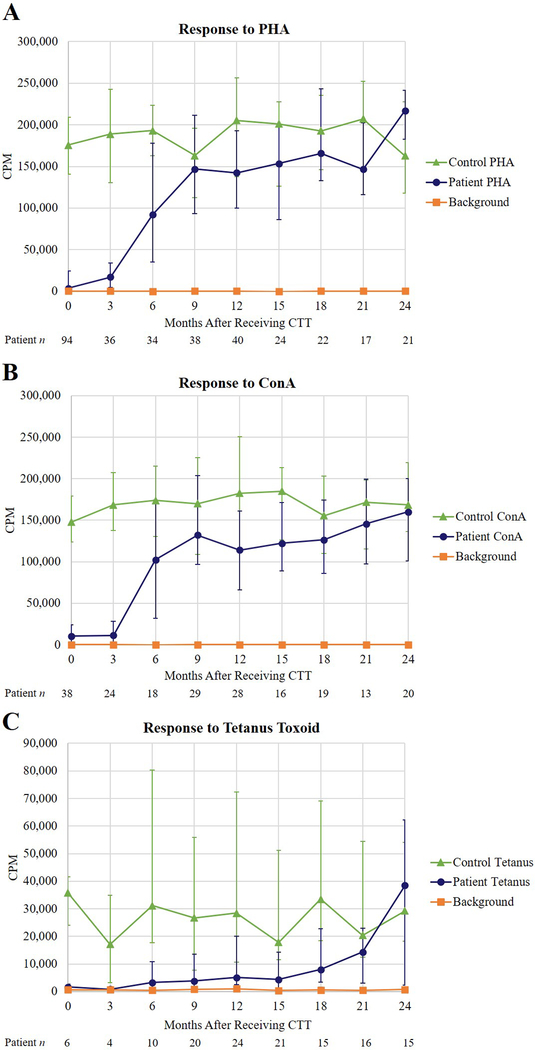
Methods: A total of 10 prospective, single-arm open-label studies with patient enrollment from 1993 to 2020 form the basis of this data set. Patients were tested after administration of CTT for T-cell development; all adverse events and infections were recorded.
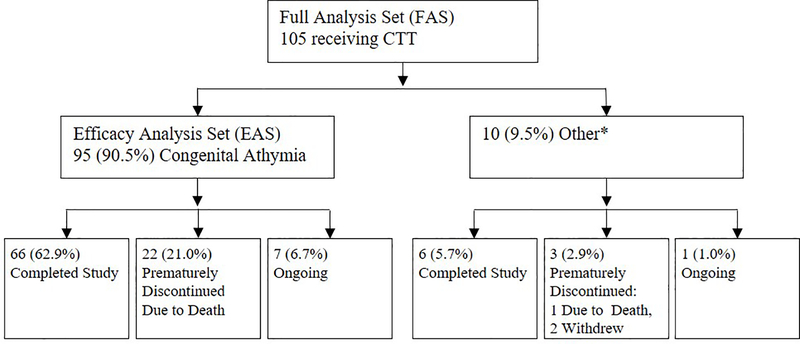
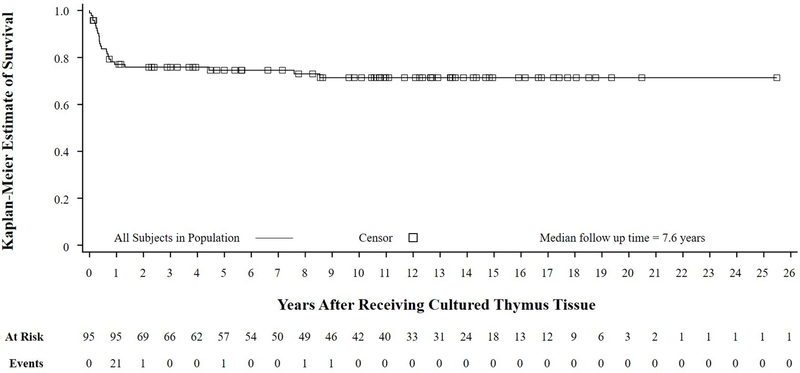
Results: A total of 105 patients were enrolled and received CTT (the full analysis set). Of those patients, 10 had diagnoses other than congenital athymia and/or received prior treatments. Of those 105 patients, 95 patients with treatment-naive congenital athymia were included in the efficacy analysis set (EAS). The Kaplan-Meier estimated survival rates at year 1 and year 2 after administration of CTT in the EAS were 77% (95% CI = 0.670-0.844) and 76% (95% CI = 0.657-0.834), respectively. In all, 21 patients died in the first year before developing naive T cells and 1 died in the second year after receipt of CTT; 3 subsequent deaths were not related to immunodeficiency. A few patients developed alopecia, autoimmune hepatitis, psoriasis, and psoriatic arthritis after year 1. The rates of infections, autologous graft-versus-host-disease manifestations, and autoimmune cytopenias all decreased approximately 1 year after administration of CTT.
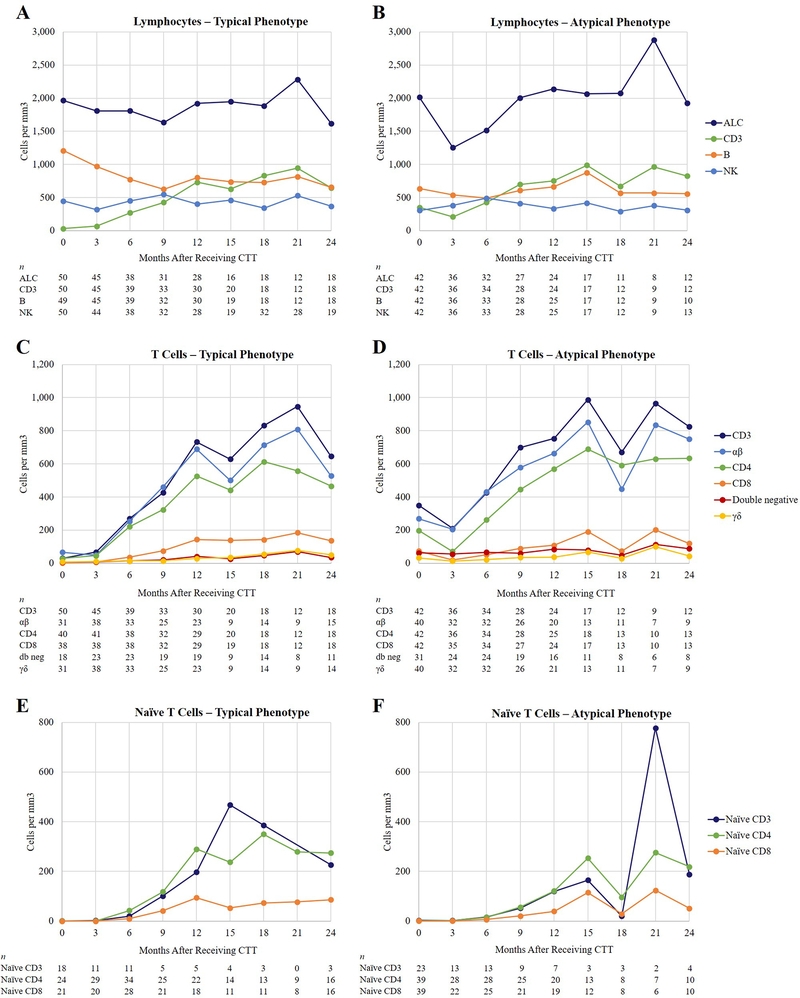
Conclusion: Treatment with CTT led to development of naive T cells with a 1-year survival rate of 77% and a median follow-up time of 7.6 years. Immune reconstitution sufficient to prevent infections and support survival typically develops 6 to12 months after administration of CTT.
Keywords: 22q11.2; CHARGE syndrome; CTT; Congenital athymia; RVT-802; complete DiGeorge; thymus transplantation.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
T Cells Prepare for a Test: Can They Tolerate a Donor Heart?Am J Transplant. 2022 Jul;22(7):1731-1732. doi: 10.1111/ajt.16663. Am J Transplant. 2022. PMID: 35789535 No abstract available.
References
-
- McDonald-McGinn DM, Sullivan KE. Chromosome 22q11.2 deletion syndrome (DiGeorge syndrome/velocardiofacial syndrome). Medicine 2011;90(1):1–18. - PubMed
-
- Markert ML, Kostyu DD, Ward FE, McLaughlin TM, Watson TJ, Buckley RH, et al. Successful formation of a chimeric human thymus allograft following transplantation of cultured postnatal human thymus. J Immunol 1997;158(2):998–1005. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
